

ADHD (aktiivisuuden ja tarkkaavuuden häiriö)
Miten viitata Käypä hoito -suositukseen? «K1»1
Keskeinen sanoma
- Aktiivisuuden ja tarkkaavuuden häiriö (attention-deficit hyperactivity disorder, ADHD) on toimintakykyä heikentävä neurokehityksellinen oireyhtymä, joka voidaan diagnosoida lapsuudessa, nuoruudessa tai aikuisuudessa.
- ADHD:n ydinoireita ovat pitkäkestoiset, ikä- ja kehitystasosta poikkeavat ja toimintakykyä haittaavat aktiivisuuden ja tarkkaavuuden vaikeudet sekä impulsiivisuus. Toiminnanohjauksen vaikeudet ovat tavallisia.
- Tukitoimet pitää aloittaa heti, kun havaitaan tarkkaavuuteen, yliaktiivisuuteen tai
impulsiivisuuteen liittyviä toiminta- tai oppimiskyvyn ongelmia. Jos tukitoimet lievittävät oireita riittävästi, tarkempia tutkimuksia ADHD:n arvioimiseksi
ei välttämättä tarvita.
- Erityistä huomiota tulee kiinnittää yleistä hyvinvointia ylläpitäviin elintapoihin (riittävä uni, liikunta, päivärytmi, ravitsemus ja sähköisen median käyttö).
- Ks. video Tukitoimet aloitetaan heti huolen herätessä «Tukitoimet aloitetaan heti huolen herätessä (video)»1.
- Haittaavien oireiden jatkuessa tehdään ensin yleinen ja systemaattinen kokonaistilanteen
ja oirekuvan arvio. Liian varhainen ADHD-oireisiin kohdentunut arviointi altistaa ADHD:n ylidiagnosoinnille
ja muiden häiriöiden ja syiden tunnistamatta jäämiselle.
- Ks. video Milloin tarvitaan ADHD-oireiden tarkempaa arviointia? «Milloin tarvitaan ADHD-oireiden tarkempaa arviointia? (video)»2.
- ADHD-oireiden arviointi aloitetaan, jos oirekuva viittaa ADHD:hen, oireet eivät selity
muilla syillä kuten elämäntilanteella tai -tavoilla ja oireista aiheutuu haittaa toimintakyvylle.
- Diagnostiseen arvioon tarvitaan tietoa oireiden esiintymisestä ja toimintakyvystä eri tilanteissa nyt ja aiemmin, henkilön psyykkisestä ja fyysisestä terveydentilasta, kehityshistoriasta, elämäntilanteesta sekä muista oireisiin vaikuttavista tekijöistä. Ks. video ADHD:n diagnosointi vaatii huolellisen arvion «ADHD:n diagnosointi vaatii huolellisen arvion (video)»3.
- Arviointi vaatii yleensä useita tapaamisia ja tiedon hankkimista eri lähteistä.
- Erilaisia oirearviointimenetelmiä kuten kyselyitä tulee käyttää vain osana laajaa kokonaisarviota
- Erotusdiagnostiikassa on arvioitava, selittyvätkö oireet muilla sairauksilla tai häiriöillä. Monet erotusdiagnostisesti olennaisista häiriöistä voivat esiintyä myös samanaikaisesti ADHD:n kanssa.
- ADHD-oireita voidaan hoitaa sekä psykososiaalisilla hoitomuodoilla että lääkehoidolla.
Hoidon tarve arvioidaan ja kuntoutuksen menetelmät suunnitellaan yksilöllisesti.
- ADHD:n hoidossa suositellaan käytettäväksi iänmukaisia psykososiaalisia menetelmiä.
- Lääkehoito voi olla tarpeen osana hoidon kokonaisuutta. Sen tarve arvioidaan diagnoosin varmistuttua, etenkin jos muut tuki- ja hoitomuodot osoittautuvat riittämättömiksi tai jos oireet ovat niin vaikeita, että muiden hoitomuotojen toteuttaminen ei onnistu. Mikäli lääkehoito aloitetaan, sen seurannan täytyy olla systemaattista ja erityisesti alussa riittävän tiivistä.
- Samanaikaisten häiriöiden hoito yhdistetään ADHD-oireiden hoitoon.
- ADHD:n ja päihdehäiriön arviointi ja hoito on pyrittävä toteuttamaan yksiköissä, joissa on osaamista molemmista häiriöistä.
- Ks. videot ADHD:n hyvä hoito vastaa yksilöllisiin tarpeisiin «ADHD:n hyvä hoito vastaa yksilöllisiin tarpeisiin (video)»4, ADHD:n lääkehoito voi olla tarpeen osana hoidon kokonaisuutta «ADHD:n lääkehoito voi olla tarpeen osana hoidon kokonaisuutta (video)»5, Päihdehäiriö ei saa estää ADHD:n tutkimista «Päihdehäiriö ei saa estää ADHD:n tutkimista (video)»6 ja ADHD:ta voidaan hoitaa samaan aikaan päihdehäiriön kanssa «ADHD:ta voidaan hoitaa samaan aikaan päihdehäiriön kanssa (video)»7.
- Hoidon on oltava riittävän pitkäjänteistä, ja sen jatkuvuus tulee varmistaa erilaisissa siirtymävaiheissa erityisesti lapsuuden ja nuoruuden aikana.
- Hoitamattomana ADHD voi haitata opintoja ja työllistymistä sekä lisätä psykiatristen häiriöiden, syrjäytymisen ja päihteiden käytön riskiä.
- Perusterveydenhuollon ja erikoissairaanhoidon välisestä työnjaosta ja yhteistyöstä
tulee sopia paikallisesti. ADHD:n diagnostiikka ja hoidon seuranta suositellaan keskitettäväksi
myös perusterveydenhuollossa neurokehityksellisiin oireyhtymiin ja niiden erotusdiagnostiikkaan
perehtyneille työntekijöille.
- Lasten ja nuorten ADHD:n diagnosointi ja hoito voidaan useimmiten toteuttaa perusterveydenhuollossa, tarvittaessa erikoissairaanhoidon konsultaatioiden tuella. Jos esiintyy vaikeita samanaikaisoireita, erotusdiagnostinen arvio ja hoito- ja kuntoutussuunnitelma tehdään erikoissairaanhoidossa.
- Aikuisten diagnoosin tekee ensisijaisesti psykiatrian erikoislääkäri tai opiskelu- tai työterveyshuollossa toimiva lääkäri, tarvittaessa konsultoimalla ADHD:n diagnostiikkaan ja hoitoon perehtynyttä erikoislääkäriä.
Tiivistelmä ja potilasversio
- Suosituksen tiivistelmä «ADHD (aktiivisuuden ja tarkkaavuuden häiriö)»1
- Suosituksen yleiskielinen potilasversio suomeksi «ADHD»2 ja ruotsiksi «ADHD»3
Aiheen rajaus
- Hoitosuositus koskee lasten, nuorten ja aikuisten ADHD:n diagnosointia, hoitoa ja kuntoutusta.
- Suosituksessa käsitellään myös hoitoa ja kuntoutusta tavallisimpien samanaikaisten häiriöiden yhteydessä.
- Kansainvälisen GRADE-työryhmän tavoitteena on ollut kehittää yhteinen, ymmärrettävä ja läpinäkyvä tapa arvioida tutkimustiedon luotettavuutta ja suositusten vahvuutta. Käypä hoito -toimituksessa GRADE-menetelmiä on otettu käyttöön vuodesta 2023 lähtien ja tavoitteena on, että uudet näytönastekatsaukset Käypä hoito -suositusten laatimisen ja päivittämisen yhteydessä laaditaan GRADE-menetelmiä soveltaen. Aiemmin julkaistuja näytönastekatsauksia emme pääsääntöisesti päivitä GRADE-menetelmien mukaan. Lisätietoa GRADE-menetelmistä, ks. «https://book.gradepro.org/»1.
Tavoitteet
- Hoitosuosituksen tavoitteena on yhtenäistää ADHD:n diagnostiikkaa, hoitoa ja kuntoutusta ja tarjota näyttöön perustuvaa tietoa hoitoratkaisujen tueksi.
- Tavoitteena on myös vastata tavallisimpiin ADHD:tä koskeviin kysymyksiin (ks. esim. «Danielson J, Mohammadi N, Espinosa-Leal L. Attenti...»1). Suositusta laadittaessa on otettu huomioon potilasviiteryhmän esittämiä näkökulmia.
Kohderyhmät
- Suositus on tarkoitettu ensisijaisesti ADHD-oireisia lapsia, nuoria ja aikuisia tutkiville, hoitaville ja kuntouttaville sosiaali- ja terveydenhuollon toimijoille.
- Suositus tarjoaa tutkittua tietoa myös ADHD-diagnoosin saaneille lapsille, nuorille ja aikuisille perheineen, varhaiskasvatuksen, koulujen ja opiskelupaikkojen henkilökunnalle ja työelämäpalveluiden ammattihenkilöille, kolmannen sektorin toimijoille sekä palvelujärjestelmiä suunnitteleville ja niistä päättäville.
Määritelmät
- Aktiivisuuden ja tarkkaavuuden häiriöstä käytetään suosituksessa vakiintunutta lyhennettä ADHD (attention-deficit hyperactivity disorder).
- Suosituksessa viitataan diagnoosien osalta kansainvälisen diagnostisen luokittelujärjestelmän (International Classification of Diseases) versioihin ICD-10 ja ICD-11 sekä Amerikan psykiatrisen yhdistyksen (APA) laatimaan psykiatristen häiriöiden DSM-5-diagnoosiluokitukseen (Diagnostic and Statistical Manual of Mental Disorders). Suomessa on tällä hetkellä virallisesti käytössä ICD-10-luokittelujärjestelmä. ICD-11 tulee käyttöön todennäköisesti vuonna 2028.
- Suosituksessa on käytetty englanninkielisestä käsitteestä cognitive behavioral therapy, CBT suomennoksena termiä kognitiivis-behavioraalinen psykoterapia tai interventio. Tätä käytetään suosituksessa kattokäsitteenä, ja se sisältää Suomessa käytetyt kognitiiviset, kognitiivis-integratiiviset ja kognitiivisen käyttäytymisterapian interventiot.
- Suosituksessa käytetty muu terminologia, tutkimuksiin liittyvä sanasto ja lääketieteellisissä teksteissä esiintyvät käsitteet löytyvät Potilasedustajien käsikirjasta Oudot sanat ja terminologiaa «Esipuhe (Potilasedustajien käsikirja)»4.
Esiintyvyys
- ADHD:n yleisyyttä voidaan tarkastella esiintyvyyden ja ilmaantuvuuden määritelmillä.
Esiintyvyys kuvaa sairastuneiden määrää tietyllä hetkellä (sairastamista), ilmaantuvuus
uusien tapausten määrää (sairastumista).
- Arviot voivat perustua läheisten tai henkilöiden itsensä ilmoittamiin oireisiin, diagnostisiin haastatteluihin tai erilaisten viranomaisrekistereiden tietoihin.
- Esiintyvyysluvut kuvaavat häiriön keskimääräistä yleisyyttä olemassa olevan tutkimustiedon
perusteella, joten niitä ei tule pitää ohjeellisena esiintyvyyden ylä- tai alarajana.
- Ikäjakauma on otettava huomioon esiintyvyysarvioita toisiinsa verrattaessa.
- Vuonna 2023 julkaistussa sateenvarjokatsauksessa ADHD:n esiintyvyydeksi lapsilla ja
nuorilla arvioitiin 8,0 % (6,0–10 %) «Ayano G, Demelash S, Gizachew Y, ym. The global pr...»2.
- Toisen vuonna 2023 julkaistun meta-analyysin mukaan ADHD:n esiintyvyydeksi 3–12-vuotiailla lapsilla arvioitiin 7,6 % (6,1–9,4 %) ja 12–18-vuotiailla 5,6 % (4,8–7 %) «Salari N, Ghasemi H, Abdoli N, ym. The global prev...»3.
- Aiemmissa, vuosina 2014–2015 tehdyissä meta-analyyseissä esiintyvyyden arvioitiin olevan 6–18-vuotiailla noin 5 % (3,6–7,2 %) «Polanczyk GV, Willcutt EG, Salum GA, ym. ADHD prev...»4, «Polanczyk GV, Salum GA, Sugaya LS, ym. Annual rese...»5, «Thomas R, Sanders S, Doust J, ym. Prevalence of at...»6.
- Suomessa vuonna 2023 esiintyvyys oli 7–12-vuotiailla pojilla 11,3 % ja tytöillä 3,9 %, nuoruusikäisillä pojilla 9,5 % ja tytöillä 5,7 % «Vuori M, Paavilainen M, Vuorenmaa M, Tuovinen E, A...»7.
- Esiintyvyyden on arvioitu olevan aikuisilla 2,2–3,4 % «Fayyad J, De Graaf R, Kessler R, ym. Cross-nationa...»8, «Fayyad J, Sampson NA, Hwang I, ym. The descriptive...»9, «Song P, Zha M, Yang Q, ym. The prevalence of adult...»10.
- Iän myötä ADHD:n esiintyvyys pienenee «Song P, Zha M, Yang Q, ym. The prevalence of adult...»10, «Faraone SV, Banaschewski T, Coghill D, ym. The Wor...»11. Meta-analyysi arvioi ADHD:n esiintyvyyden olevan yli 50-vuotiailla 2,2 %, kun käytettiin validoituja mittareita, ja 0,2 %, kun käytettiin kliinistä diagnoosia «Dobrosavljevic M, Solares C, Cortese S, ym. Preval...»12.
- Suomessa ADHD:n esiintyvyys vuonna 2022 oli 21–30-vuotialla miehillä 3,9 % ja naisilla 2,6 %, 31–55-vuotiailla vastaavasti 1,3 % ja 1,2 % ja sitä vanhemmilla 0,1 % ja 0,1 % «Auro K, Holopainen I, Perola M, ym. Attention-Defi...»13.
- Kaikki suosituksen valmistumiseen mennessä Suomessa tehdyt ADHD:n esiintyvyyttä tai lääkehoidon yleisyyttä koskevat tutkimukset on koottu taulukkomuotoiseen lisätietoaineistoon «ADHD:n ja lääkehoidon yleisyyttä koskevat tutkimukset Suomessa»8.
- ADHD-diagnoosin pysyvyys lapsuudesta aikuisuuteen on eri tutkimuksissa ollut 4–77
% «Sibley MH, Mitchell JT, Becker SP. Method of adult...»14 riippuen muun muassa käytetyistä informaatiolähteistä, menetelmistä sekä eroista
oireiden ja niistä koituvan haitan arvioinnissa. Laadukkaimpien tutkimusten mukaan
pysyvyys oli noin 40–50 %.
- Vuonna 2021 julkaistu meta-analyysi arvioi lapsuudesta aikuisuuteen jatkuvan (lapsuudessa todetun ja aikuisuudessa edelleen diagnoosikriteerit täyttävän) ADHD:n esiintyvyydeksi 2,6 % «Song P, Zha M, Yang Q, ym. The prevalence of adult...»10. Tätä tuoreempi meta-analyysi arvioi esiintyvyydeksi 3,1 % «Ayano G, Demelash S, Gizachew Y, ym. The global pr...»2.
- ADHD-diagnoosi on yleisempi lapsuudessa pojilla kuin tytöillä, mutta ero tasoittuu
iän myötä «Auro K, Holopainen I, Perola M, ym. Attention-Defi...»13, «Simon V, Czobor P, Bálint S, ym. Prevalence and co...»15.
- Väestöpohjaisissa tutkimuksissa poikien ja tyttöjen välinen suhde on ollut jopa 5:1 «Joelsson P, Chudal R, Gyllenberg D, ym. Demographi...»16, «Polanczyk G, de Lima MS, Horta BL, ym. The worldwi...»17, «Ramtekkar UP, Reiersen AM, Todorov AA, ym. Sex and...»18, «Rucklidge JJ. Gender differences in attention-defi...»19.
- Ruotsalaisessa väestörekisteritutkimuksessa todettiin, että naiset saivat ADHD-diagnoosin noin 4 vuotta myöhemmin kuin miehet (ikä 23,5 vuotta vs. 19,6 vuotta) «Skoglund C, Sundström Poromaa I, Leksell D, ym. Ti...»20.
- Suomalaisissa rekisteritutkimuksissa ADHD-diagnoosien ilmaantuvuuden todettiin olevan
suurinta nuoruusikäisillä tytöillä «Vuori M, Paavilainen M, Vuorenmaa M, Tuovinen E, A...»7, «Auro K, Holopainen I, Perola M, ym. Attention-Defi...»13.
- Vuoden 2023 kouluterveyskyselyssä 8–9-luokkalaisten ilmoittamien keskittymisvaikeuksien yleisyys oli kaikilla hyvinvointialueilla suurempi tytöillä (20,3–26,3 %) kuin pojilla (8,6–11,7 %). Ahvenanmaalla ero oli vähäisempi (tytöillä 26,7 % ja pojilla 18,5 %).
- Kansainvälinen meta-analyysi totesi ADHD:n esiintyvyyden psykiatrisissa avopalveluissa asioivien joukossa olevan 14–27 %, eikä sukupuolien välisiä eroja ollut «Adamis D, Flynn C, Wrigley M, ym. ADHD in Adults: ...»21.
- Suurissa rekisteriaineistoihin perustuvissa tutkimuksissa on havaittu, että luokka-
ja kasvatusryhmänsä nuorimmat lapset saavat ADHD-diagnoosin ja myös lääkehoitoa useammin
kuin vanhimmat «Whitely M, Raven M, Timimi S, ym. Attention defici...»22, «Vuori M, Martikainen JE, Koski-Pirilä A, ym. Child...»23. Ks. lisätietoa «Suhteellisen iän yhteys ADHD-diagnoosiin ja lääkehoitoon»9. Yhteys suhteelliseen ikään on ollut vahvin nuorimmissa, juuri koulun aloittaneissa
ikäluokissa «Vuori M, Martikainen JE, Koski-Pirilä A, ym. Child...»23.
- Tutkimukset eivät suoraan kerro, onko kyseessä
- ADHD:hen liittyvä aivotoimintojen kypsymisen hitaus, jonka vaikutuksia ikäero ryhmän vanhimpien ja nuorimpien välillä korostaa
- muiden kehityksellisten ongelmien tulkinta ADHD:stä johtuviksi
- lapseen kohdistuvien odotusten kohtuuttomuus vai
- vuosiluokan nuorimpien ADHD:n ylidiagnosointi.
- Tutkimukset eivät suoraan kerro, onko kyseessä
- ADHD-diagnoosien ja lääkehoidon määrä on yleistynyt voimakkaasti viime vuosina maailmanlaajuisesti
«Salari N, Ghasemi H, Abdoli N, ym. The global prev...»3, «Song P, Zha M, Yang Q, ym. The prevalence of adult...»10, myös Suomessa, ks. «Vuori M, Martikainen JE, Koski-Pirilä A, ym. Child...»23, «Auro K, Holopainen I, Perola M, ym. Attention-Defi...»13, «Vuori M, Vuorenmaa M, Ervasti E, Tuovinen E, Aalto...»24 ja lisätietoa «ADHD:n ja lääkehoidon yleisyyttä koskevat tutkimukset Suomessa»8.
- Luotettavaa tutkimustietoa esiintyvyyden lisääntymisen syistä ei ole julkaistu
- Esiintyvyyden lisääntymisessä kyse voi olla
- aiempien esiintyvyystutkimusten todellista pienemmistä esiintyvyysarvioista (esimerkiksi tutkimusmetodeihin liittyen) «Ayano G, Demelash S, Gizachew Y, ym. The global pr...»2
- lisääntyneestä ADHD:n tunnistamisesta ja diagnosoinnista «Faraone SV, Banaschewski T, Coghill D, ym. The Wor...»11. On mahdollista, että diagnoosit kohdentuvat aiempaa enemmän lieväoireisiin tapauksiin «Kazda L, Bell K, Thomas R, ym. Attention deficit/h...»25.
- tyttöjen ja naisten ADHD:n paremmasta tunnistamisesta. Uudemmissa tutkimuksissa erityisesti nuoruusikäisten tyttöjen diagnoosien määrä on lisääntynyt «Auro K, Holopainen I, Perola M, ym. Attention-Defi...»13, «Westman E, Prami T, Kallio A, ym. Increase in Occu...»26.
- hoitokulttuurin muutoksesta, jossa diagnoosi asetetaan madaltunein tai riittämättömin kriteerein «Kazda L, Bell K, Thomas R, ym. Attention deficit/h...»25, ks. myös lisätietoa Voiko ADHD-diagnoosista olla lapsille ja nuorille haittaa? «Voiko ADHD-diagnoosista olla lapsille ja nuorille haittaa?»10.
- virhediagnostiikasta, jolloin oireiden taustalla onkin jokin muu syy tai häiriö, ks. lisätietoa Voiko ADHD-diagnoosista olla lapsille ja nuorille haittaa? «Voiko ADHD-diagnoosista olla lapsille ja nuorille haittaa?»10.
- ADHD:n esiintyvyyden (tuntemattomasta syystä johtuvasta) todellisesta lisääntymisestä.
- Keskittymiskyvyn kehittymiseen vaikuttavilla lapsuudenaikaisilla tekijöillä sekä ympäristön
vaikutuksella on epäilty olevan merkitystä keskittymisvaikeuksien ja koettujen ADHD-oireiden
yleistymiseen. Tällaisia ovat esimerkiksi
- älylaitteiden käyttö «Montagni I, Guichard E, Kurth T. Association of sc...»27, «Ra CK, Cho J, Stone MD, ym. Association of Digital...»28, pitkäjänteisen keskittymisen harjoittelun vähäisyys ja muutokset kouluympäristössä ja opetusmetodeissa
- altistuminen sosiaalisen median vaikuttajien jakamalle ADHD-aiheiselle tiedolle sekä erilaiset itsearviointikyselyt «Yeung A, Ng E, Abi-Jaoude E. TikTok and Attention-...»29, «Verma S, Sinha SK. How evidence-based is the "hash...»30.
- Esiintyvyyden lisääntyminen ja huomattavat alueelliset erot korostavat huolellisen diagnosoinnin tärkeyttä.
Etiologia ja riskitekijät
- ADHD on lapsuudessa alkava neurokehityksellinen oireyhtymä.
- ADHD:n tausta on monitekijäinen, ja sen ilmenemiseen vaikuttavat yhdessä erilaiset perimän ja ympäristön altistavat ja suojaavat tekijät. Monimuotoinen tausta selittää myös ADHD:n monimuotoisen ilmiasun «Faraone SV, Banaschewski T, Coghill D, ym. The Wor...»11, «Faraone SV, Larsson H. Genetics of attention defic...»31, «Sonuga-Barke EJS, Becker SP, Bölte S, ym. Annual R...»32, «Thapar A, Cooper M. Attention deficit hyperactivit...»33, «Nigg J, Nikolas M, Burt SA. Measured gene-by-envir...»34, «van der Meer D, Hoekstra PJ, Bralten J, ym. Interp...»35.
Genetiikka
- Kaksos- ja perhetutkimukset ovat osoittaneet alttiuden ADHD:lle olevan voimakkaasti
periytyvää. Arviot periytyvän komponentin osuudesta vaihtelevat välillä 74–88 % «Faraone SV, Larsson H. Genetics of attention defic...»31
- ADHD-oireisten henkilöiden ensimmäisen asteen sukulaisilla esiintyy ADHD:tä 2–8 kertaa useammin kuin väestöllä keskimäärin «Chen Q, Brikell I, Lichtenstein P, ym. Familial ag...»36, «Brikell I, Burton C, Mota NR, ym. Insights into at...»37.
- ADHD:n periytyvä komponentti on samaa suuruusluokkaa riippumatta sukupuolesta, oirekuvasta, oirekuvan vaikeusasteesta tai ADHD:n kehityskulusta «Sonuga-Barke EJS, Becker SP, Bölte S, ym. Annual R...»32, «Brikell I, Burton C, Mota NR, ym. Insights into at...»37.
- Aikuisiän ADHD:n periytyvyys vaikuttaisi olevan samaa suuruusluokkaa kuin lapsuusiän ADHD:n «Faraone SV, Larsson H. Genetics of attention defic...»31, «Ribasés M, Mitjans M, Hartman CA, ym. Genetic arch...»38.
- Samat geneettiset tekijät selittävät jatkumona sekä väestötasolla ilmeneviä ADHD-piirteitä
että diagnostiset kriteerit täyttävää ADHD:tä «Faraone SV, Larsson H. Genetics of attention defic...»31, «Sonuga-Barke EJS, Becker SP, Bölte S, ym. Annual R...»32, «Ribasés M, Mitjans M, Hartman CA, ym. Genetic arch...»38, «Demontis D, Walters GB, Athanasiadis G, ym. Genome...»39, ks. lisätietoa «ADHD:n periytyvyys ja genetiikka»11.
- ADHD:llä on myös yhteisiä geneettisiä alttiustekijöitä muiden neurokehityksellisten oireyhtymien, mielialahäiriöiden, autismikirjon häiriön, käytöshäiriöiden ja skitsofrenian kanssa «Demontis D, Walters GB, Athanasiadis G, ym. Genome...»39, «Cole J, Ball HA, Martin NC, ym. Genetic overlap be...»40, «Thapar A, Cooper M, Eyre O, ym. What have we learn...»41, «Cross-Disorder Group of the Psychiatric Genomics C...»42, «Thapar A. Discoveries on the Genetics of ADHD in t...»43, «Andersson A, Tuvblad C, Chen Q, ym. Research Revie...»44, «Kittel-Schneider S, Arteaga-Henriquez G, Vasquez A...»45.
- Geenitutkimuksista ei ole hyötyä ADHD:n diagnostiikassa, eikä niitä tule siinä tarkoituksessa
käyttää (esim. «Grimm O, Kranz TM, Reif A. Genetics of ADHD: What ...»46).
- Yksittäisen henkilön ADHD-diagnoosin yhdistäminen havaittuun perimän muutokseen on hyvin epävarmaa, ja etenkään diagnoosin ennustaminen geenitutkimusten perusteella ei ole luotettavaa (esim. «Sonuga-Barke EJS, Becker SP, Bölte S, ym. Annual R...»32, «Brikell I, Burton C, Mota NR, ym. Insights into at...»37, «Grimm O, Kittel-Schneider S, Reif A. Recent develo...»47).
Raskaudenaikaiset ympäristötekijät ja synnynnäiset rakenteelliset tekijät
- Pre- ja perinataalinen hapenpuute, hyvin pieni syntymäpaino, synnytyskomplikaatiot, vastasyntyneen hapenpuute ja veren pieni glukoosipitoisuus saattavat suurentaa yliaktiivisuuden ja neuropsykiatristen kehityshäiriöiden, kuten oppimisvaikeuksien ja tarkkaavuuden häiriöiden, riskiä «Thapar A, Cooper M, Eyre O, ym. What have we learn...»41, «Smith TF, Schmidt-Kastner R, McGeary JE, ym. Pre- ...»48, «Bitsko RH, Holbrook JR, O'Masta B, ym. A Systemati...»49, «Robinson R, Girchenko P, Pulakka A, ym. ADHD sympt...»50.
- Sikiöaikainen altistuminen äidin tupakoinnille «Neuman RJ, Lobos E, Reich W, ym. Prenatal smoking ...»51, «Joelsson P, Chudal R, Talati A, ym. Prenatal smoki...»52, «Langley K, Rice F, van den Bree MB, ym. Maternal s...»53, «Biederman J, Petty CR, Bhide PG, ym. Does exposure...»54, «Haan E, Westmoreland KE, Schellhas L, ym. Prenatal...»55, «Huang L, Wang Y, Zhang L, ym. Maternal Smoking and...»56 tai alkoholin tai huumeiden käytölle «Nygaard E, Slinning K, Moe V, ym. Behavior and Att...»57, «Knopik VS, Sparrow EP, Madden PA, ym. Contribution...»58, «Brookes KJ, Mill J, Guindalini C, ym. A common hap...»59 on yhteydessä ADHD:n riskiin ainakin niillä lapsilla, jotka ovat siihen geneettisesti
alttiita. Myös tupakoimattoman äidin sikiö voi altistua tupakoinnille erimerkiksi
isän tupakoinnin tai äidin työperäisen altistuksen vuoksi «Han JY, Kwon HJ, Ha M, ym. The effects of prenatal...»60.
- Raskauden aikana tupakoivien äitien lapsilla on muita lapsia enemmän ADHD-oireita. Osa tästä erosta selittyy myös periytyvyydellä (ks. lisätietoa «Äidin tupakoinnin vaikutus lapsen ADHD-riskiin»12).
- Altistuminen alkoholille raskauden aikana aiheuttaa lapselle haitallisia vaikutuksia (fetal alcohol spectrum disorders, FASD). Niihin liittyy ADHD-tyyppisiä oireita, muun muassa toiminnanohjauksen puutteita, tarkkaamattomuutta ja yliaktiivisuutta (ks. lisätietoa «Sikiöaikaisen alkoholialtistuksen vaikutus lapsen kehittymiseen ja ADHD-riskiin»13).
- Sikiöaikana kokaiinille, kannabikselle tai keskushermostoon vaikuttavien lääkkeiden päihdekäytölle altistuneilla lapsilla on suurentunut tarkkaavuuden ylläpitämisen ja käyttäytymisen säätelyn vaikeuksien riski. Monilla heistä oireet yltävät ADHD-diagnoosiin saakka «Ackerman JP, Riggins T, Black MM. A review of the ...»61, «Noland JS, Singer LT, Short EJ, ym. Prenatal drug ...»62, «Huizink AC, Mulder EJ. Maternal smoking, drinking ...»63, «Elgen I, Bruaroy S, Laegreid LM. Complexity of foe...»64.
- Äidin ylipaino ennen raskauden alkua ja raskauden aikana suurentaa lapsen ADHD:n riskiä «Li L, Lagerberg T, Chang Z, ym. Maternal pre-pregn...»65, «Nilsson IAK, Ozsvar J, Gissler M, ym. Maternal Eat...»66, «Duko B, Mengistu TS, Stacey D, ym. Associations be...»67.
- Äidin raskaudenaikainen stressi suurentaa syntyvän lapsen stressiherkkyyttä sekä ADHD:n, ahdistuneisuuden ja masennuksen riskiä «Van den Bergh BRH, van den Heuvel MI, Lahti M, ym....»68, «Okano L, Ji Y, Riley AW, ym. Maternal psychosocial...»69, «Jallow J, Hurtig T, Kerkelä M, ym. Prenatal matern...»70.
Psykososiaaliset riskitekijät
- Varhaisten psykososiaalisten ympäristötekijöiden suorasta syy-yhteydestä ADHD:n kehittymiseen
on hyvin vähän tutkimusnäyttöä «Humphreys KL, Zeanah CH. Deviations from the expec...»71.
- Vaikeille varhaisille kaltoinkohtelukokemuksille, kuten äärimmäisen vähävirikkeiselle laitosympäristölle, altistuneilla lapsilla on kuitenkin todettu myöhemmin muita enemmän tarkkaamattomuus-ylivilkkausoireita «Golm D, Sarkar S, Mackes NK, ym. The impact of chi...»72.
- Perheolosuhteisiin liittyvät riskitekijät voivat vaikuttaa negatiivisesti keskushermoston
kehitykseen tai vaikeuttaa turvallisen kiintymyssuhteen muodostumista sekä motoriikan
ja vireyden säätelytaitojen kehittymistä erityisesti varhaislapsuudessa «Wylock JF, Borghini A, Slama H, ym. Child attachme...»73, «Storebø OJ, Rasmussen PD, Simonsen E. Association ...»74, «Al-Yagon M, Forte D, Avrahami L. Executive Functio...»75, «Pallini S, Morelli M, Chirumbolo A, ym. Attachment...»76.
- Epäjohdonmukainen ja rankaiseva kasvatus, kielteinen perheilmapiiri, väkivaltakokemukset sekä vanhempien psyykkiset sairaudet, kuten äidin masennus ja vanhemman oma ADHD, lisäävät samanaikaissairastavuuden, esimerkiksi käytöshäiriöiden, kehittymisen riskiä «Claussen AH, Holbrook JR, Hutchins HJ, ym. All in ...»77, «Deault LC. A systematic review of parenting in rel...»78, «Park JL, Hudec KL, Johnston C. Parental ADHD sympt...»79, «Robinson LR, Bitsko RH, O'Masta B, ym. A Systemati...»80.
Sähköinen media
- Sähköisen median käyttö voi vaikuttaa aktiivisuuden ja tarkkaavuuden vaikeuksiin.
- Alle kouluikäisten runsas altistuminen sähköiselle medialle voi heikentää säätelytaitojen
kehitystä, etenkin jos unen, liikunnan, leikin ja vuorovaikutuksen määrä vähenee.
Runsas sähköisen median käyttö on liitetty muun muassa kielen kehityksen viiveisiin,
keskittymisen vaikeuksiin, levottomuuteen, autismikirjon häiriöön ja käytösoireisiin
«Niiranen J, Kiviruusu O, Vornanen R, ym. Children'...»81, «Radesky JS, Kaciroti N, Weeks HM, ym. Longitudinal...»82, «Anitha FS, Narasimhan U, Janakiraman A, ym. Associ...»83, «Girela-Serrano BM, Spiers ADV, Ruotong L, ym. Impa...»84. WHO:n suosituksen mukaan alle 2-vuotiailla ei tulisi olla lainkaan ruutuaikaa ja
alle kouluikäisillä korkeintaan yksi tunti päivässä «Guidelines on physical activity, sedentary behavio...»85.
- Myös vanhemman runsas älylaitteiden käyttö voi haitata lapsen kehitystä, sillä se vähentää vuorovaikutusta «Lederer Y, Artzi H, Borodkin K. The effects of mat...»86. Aikuisten tulee myös toimia esimerkkinä älylaitteiden järkevässä ja kohtuullisessa käytössä.
- Myös mediasisältöihin on syytä kiinnittää huomiota, sillä monet lastenohjelmatkin voivat lisätä levottomuutta.
- Alle kouluikäisten runsas altistuminen sähköiselle medialle voi heikentää säätelytaitojen
kehitystä, etenkin jos unen, liikunnan, leikin ja vuorovaikutuksen määrä vähenee.
Runsas sähköisen median käyttö on liitetty muun muassa kielen kehityksen viiveisiin,
keskittymisen vaikeuksiin, levottomuuteen, autismikirjon häiriöön ja käytösoireisiin
«Niiranen J, Kiviruusu O, Vornanen R, ym. Children'...»81, «Radesky JS, Kaciroti N, Weeks HM, ym. Longitudinal...»82, «Anitha FS, Narasimhan U, Janakiraman A, ym. Associ...»83, «Girela-Serrano BM, Spiers ADV, Ruotong L, ym. Impa...»84. WHO:n suosituksen mukaan alle 2-vuotiailla ei tulisi olla lainkaan ruutuaikaa ja
alle kouluikäisillä korkeintaan yksi tunti päivässä «Guidelines on physical activity, sedentary behavio...»85.
- Runsas digilaitteiden ja sosiaalisen median käyttö, television katsominen ja videopelit saattavat lisätä nuorten ADHD-oireiden riskiä. Haitalliset vaikutukset voivat liittyä ainakin osittain sähköisen median koukuttavuuteen ja siitä seuraavaan impulssikontrollin heikkenemiseen ja monisuorittamiseen (multitasking). Ks. lisätietoa «Sähköinen media ja ADHD-oireet»14, «Kosola S. Lasten ja nuorten netti- ja peliriippuvu...»87, «Dekkers TJ, van Hoorn J. Understanding Problematic...»88.
- Runsas älypuhelimen käyttö liittyy vähäisempään unen määrään ja huonompaan unen tehokkuuteen, mikä myös voi heikentää keskittymistä ja kognitiivista toimintakykyä. Runsas älypuhelimen ja sosiaalisen median käyttö on liitetty myös ahdistukseen, masennukseen, itsetuhoisuuteen, käytösoireisiin ja syömishäiriöihin «Christensen MA, Bettencourt L, Kaye L, ym. Direct ...»89, «Ferguson CK, Branley-Bell D, ym. Screen Media an...»90, «Nan YQ, Li Z, ym. Is Social Media Use Related to ...»91.
- Jatkuvat keskeytykset, esimerkiksi sosiaalisen median tai sähköpostin merkkiäänet,
voivat häiritä keskittymistä. Henkilöt, joilla on impulssikontrollin tai tarkkaavuuden
vaikeuksia, saattavat olla muita alttiimpia näille häiriöille «Liebherr MS, Antons S, Montag C, Brand M. Smartpho...»92. Ks. lisätietoa «Keskittymisen vaikeuksia, prosessoinnin kuormittumista vai ”ADT” aikuisilla?»15.
- Sosiaalisen median oireiden itsearviointimenetelmät ja tieto ADHD:stä ovat usein harhaanjohtavia «Yeung A, Ng E, Abi-Jaoude E. TikTok and Attention-...»29, «Verma S, Sinha SK. How evidence-based is the "hash...»30. Tämä voi lisätä itse raportoitujen oireiden määrää.
Keskushermoston toiminnalliset ja rakenteelliset löydökset
- Aivojen rakenteessa ja toiminnassa on eroa ryhmätasolla, kun ADHD-diagnoosin saaneita
verrataan verrokkeihin. Tutkimuksilla ei kuitenkaan ole riittävästi pystytty selvittämään
ADHD:n patofysiologiaa. Eroja on niillä alueilla ja niissä toiminnallisissa verkostoissa,
jotka osallistuvat tarkkaavuuden ja toiminnanohjauksen toimintoihin (ks. tarkemmin
lisätietoa «ADHD ja aivojen kuvantamistutkimukset»16).
- Erot eivät kuitenkaan riitä yksittäisten henkilöiden diagnostiikkaan.
- Rakenteelliset ja toiminnalliset löydökset ovat olleet stimulanttihoitoa saaneiden ryhmässä lähempänä verrokkeja kuin hoitoa saamattomien ryhmässä «Rubia K, Alegría AA, Brinson H. Brain abnormalitie...»93, «Nakao T, Radua J, Rubia K, ym. Gray matter volume ...»94, «Frodl T, Skokauskas N. Meta-analysis of structural...»95 «Spencer TJ, Brown A, Seidman LJ, ym. Effect of psy...»96, «Hoogman M, Bralten J, Hibar DP, ym. Subcortical br...»97. Tutkimuksissa ei ole näyttöä siitä, että stimulanttihoito vaarantaisi aivojen kypsymistä «Hoogman M, Muetzel R, Guimaraes JP, ym. Brain Imag...»98.
Kliininen oirekuva
- ADHD:n ydinoireita ovat pitkäkestoiset ja toimintakykyä haittaavat aktiivisuuden ja
tarkkaavuuden säätelyn vaikeudet sekä impulsiivisuus, jotka poikkeavat ikä- ja kehitystasosta.
- Aktiivisuuden säätelyn vaikeus tarkoittaa kyvyttömyyttä säätää omaa aktiivisuutta ja toimintaa tilanteeseen sopivaksi. Tavallisimmin se ilmenee yliaktiivisuutena, esimerkiksi fyysisenä vilkkautena ja levottomuutena, nuorilla ja aikuisilla joskus vain levottomuuden tunteena. Liian vähäinen aktiivisuus voi ilmetä esimerkiksi vaikeutena aloittaa toimintaa ja hitautena.
- Tarkkaavuuden säätelyn vaikeus (vaikeus kohdentaa, ylläpitää ja siirtää tarkkaavuutta) voi ilmetä esimerkiksi keskittymisvaikeuksina, häiriöherkkyytenä, yksityiskohtien huomiotta jättämisenä, taipumuksena hukata tavaroita ja lyhytjänteisyytenä.
- Impulsiivisuus voi ilmetä esimerkiksi kärsimättömyytenä ja taipumuksena toimia nopeasti ja harkitsemattomasti, liiallisena puheliaisuutena sekä vaikeutena odottaa omaa vuoroa esimerkiksi keskusteluissa. Impulsiivisuus voi ilmetä myös tarpeettomien riskien ottamisena esimerkiksi liikenteessä.
- Tarkkaamattomuutta, aktiivisuuden säätelyn vaikeuksia ja impulsiivisuutta ilmenee ajoittain kaikilla henkilöillä, ja ero ADHD:hen tehdään oireiden pitkäkestoisuuden, vaikeusasteen ja aiheuttaman haitan perusteella. Keskittymisen vaikeuksista ilman ADHD:tä ks. lisätietoa «Keskittymisen vaikeuksia, prosessoinnin kuormittumista vai ”ADT” aikuisilla?»15.
- Usein yliaktiivisuus- ja impulsiivisuusoireet lievittyvät lapsuudesta nuoruuteen tultaessa.
Tarkkaamattomuusoireet jatkuvat yliaktiivisuusoireita useammin aikuisuuteen «Faraone SV, Biederman J, Mick E. The age-dependent...»99, «Kessler RC, Green JG, Adler LA, ym. Structure and ...»100
- Oireista saattaa aikuisuudessa olla merkittävää haittaa yksilöön kohdistuvien vaatimusten lisääntyessä, vaikka diagnoosikriteerit eivät enää täysin täyttyisi «Faraone SV, Biederman J, Mick E. The age-dependent...»99.
- Oirekuvaan liittyy tyypillisesti toiminnanohjauksen vaikeuksia esimerkiksi tehtävien suunnittelussa, aloittamisessa ja järjestelmällisessä loppuun saattamisessa, ajankäytössä ja järjestyksen ylläpitämisessä, ks. myös lisätietoa Toiminnanohjauksen ongelmat ja ADHD «Toiminnanohjauksen ongelmat ja ADHD»17.
- ADHD:hen voi kaikenikäisillä liittyä myös sosiaalisten taitojen ja tunteiden säätelyn vaikeuksia «Graziano PA, Garcia A. Attention-deficit hyperacti...»101, «Corbisiero S, Mörstedt B, Bitto H, ym. Emotional D...»102, «Vuori M, Autti-Rämö I, Junttila N, ym. Discrepanci...»103. Tunnesäätelyn vaikeudet voivat ilmetä esimerkiksi ärsyyntymisherkkyytenä, voimakkaina tunnepurkauksina sekä vaikeutena ilmaista tunnekokemuksia sosiaalisesti sopivalla tavalla «Shaw P, Stringaris A, Nigg J, ym. Emotion dysregul...»104.
- Kaikkien riippuvuuksien esiintyvyys on suurentunut henkilöillä, joilla on ADHD. Päihdehäiriöiden (ks. kohta ADHD ja päihdehäiriöt «A1»2) lisäksi on syytä muistaa myös toiminnalliset riippuvuudet «Findon JL, Muck A, Tóthpál-Davison B, ym. Investig...»105, ks. Käypä hoito -suositus Rahapeliongelma «Rahapeliongelma»5, «Rahapeliongelma. Käypä hoito -suositus. Suomalaise...»106).
- Oireiden ilmeneminen, kliininen oirekuva ja oireista aiheutuva haitta vaihtelevat
eri ikä- ja kehitysvaiheissa:
- oireet lapsilla «ADHD:n oireet lapsilla»18
- oireet nuorilla «ADHD:n oireet nuoruusikäisillä»19
- oireet aikuisilla ja ikääntyneillä «ADHD:n oireet aikuisuudessa ja ikääntyvillä»20.
- Sukupuolella on epäilty olevan vaikutusta ADHD-oireiden ilmenemiseen.
- Vuonna 2024 julkaistun meta-analyysin mukaan pojilla näyttää oirekyselyihin perustuvissa tutkimuksissa olevan enemmän yliaktiivisuusoireita kuin tytöillä. Aikuisilla eroa sukupuolten välillä ei ole yliaktiivisuus-impulsiivisuusoireissa, mutta miehillä on enemmän tarkkaamattomuusoireita. Kliiniseen arvioon perustuvissa tutkimuksissa oireiden painottumisessa ei havaittu sukupuolten välistä eroa lapsilla eikä aikuisilla «Young S, Uysal O, Kahle J, ym. A systematic review...»107.
- Hormonikierron on epäilty voivan vaikuttaa naisten ADHD-oireiden ilmenemiseen niin, että oireet vaikeutuvat ovulaation ja kuukautisten välisenä aikana «Eng AG, Nirjar U, Elkins AR, ym. Attention-deficit...»108, «Bürger I, Erlandsson K, Borneskog C. Perceived ass...»109. Tutkimustietoa sukupuolihormonien merkityksestä ADHD-oireiden ilmenemiseen ja hoitoon on kuitenkin niukasti, eikä sen perusteella ole vielä mahdollista luotettavasti arvioida asiaa «Camara B, Padoin C, Bolea B. Relationship between ...»110.
- Ympäristö- ja motivaatiotekijät sekä tukitoimet vaikuttavat oireiden määrään ja haittaavuuteen (ks. lisätietoa «ADHD-oireisiin vaikuttavat ympäristö- ja motivaatiotekijät»21). Ympäristö- ja motivaatiotekijät on syytä ottaa huomioon suhteutettaessa oireita
kontekstiin sekä tukitoimien järjestämisessä.
- Oireet ovat usein
- voimakkaampia, jos ympäristössä on paljon häiriötekijöitä, toimintaodotukset ovat epäselviä tai vaaditaan pitkäkestoista ponnistelua
- lievempiä tai eivät ilmene, jos ympäristö on rauhallinen, vireyttä ylläpitävä liikehtiminen on sallittua, ohjeet ovat selkeitä ja lyhyitä, motivaatio tekemiseen on hyvä ja palaute on välitöntä.
- Onnistuneet tukitoimet vähentävät oireiden aiheuttamaa haittaa, minkä vuoksi lapsuusiän oireita jälkeenpäin arvioitaessa on selvitettävä myös tukitoimien määrä, toteutuminen ja vaikutus.
- Oireet ovat usein
- Ryhmätason tutkimuksissa ADHD-oireiset suoriutuvat verrokkeja heikommin useita kognitiivisia toimintoja «Onandia-Hinchado I, Pardo-Palenzuela N, Diaz-Oruet...»111, «Frazier TW, Demaree HA, Youngstrom EA. Meta-analys...»112, erityisesti toiminnanohjausta «Sadozai AK, Sun C, Demetriou EA, ym. Executive fun...»113, «Boonstra AM, Oosterlaan J, Sergeant JA, ym. Execut...»114, tarkkaavuuden ylläpitämistä «Frazier TW, Demaree HA, Youngstrom EA. Meta-analys...»112 ja työmuistia «Alderson RM, Kasper LJ, Hudec KL, ym. Attention-de...»115, «Ramos AA, Hamdan AC, Machado L. A meta-analysis on...»116, mittaavissa testeissä (ks. lisätietoa «Toiminnanohjauksen ongelmat ja ADHD»17).
Diagnoosikriteerit
- Suomessa käytössä olevan ICD-10-järjestelmän diagnostisen määritelmän mukaan ADHD-diagnoosin edellytyksenä ovat kehitystasosta poikkeavat ja haittaa aiheuttavat keskittymisen, aktiivisuuden säätelyn ja impulssikontrollin ongelmat, jotka ovat pitkäkestoisia, esiintyvät useissa tilanteissa eivätkä selity paremmin muilla häiriöillä, kuten autismikirjon, mieliala- tai ahdistushäiriöillä (ICD-10). Ks. taulukko «ICD-10:n mukaiset Aktiivisuuden ja tarkkaavuuden häiriön (F90.0) diagnoosikriteerit. Kriteerien kieliasua on selkeyden lisäämiseksi hieman muokattu (alkuperäiset suomenkieliset kriteerit on esitetty lisätietoaineistossa )....»1.
- Diagnostisessa arvioinnissa voidaan käyttää myös uudempia DSM-5- ja ICD-11-järjestelmien
määritelmiä.
- DSM-5-järjestelmän määritelmä vastaa pääpiirteissään ICD-10-määritelmää. Siinä kuitenkin 17-vuotiaiden tai sitä vanhempien ADHD-diagnoosiin riittää 5 tarkkaamattomuus- tai 5 yliaktiivisuus-impulsiivisuusoiretta ja että oireet ovat alkaneet ennen 12 vuoden ikää.
- Tuleva ICD-11-luokitus ei enää määrittele vaadittavien oireiden tarkkaa lukumäärää, vaan kuvaa keskeisiä oireita oireryhminä. Myös ICD-11:n mukaan riittää, että oireet ovat alkaneet ennen 12 vuoden ikää.
- Kaikissa määritelmissä korostetaan, että oireiden tulee poiketa kehitystasosta ja aiheuttaa haittaa useissa tilanteissa. Ks. lisätietoa eri diagnoosijärjestelmien (ICD-10, ICD-11 ja DSM-5) diagnostisista määritelmistä «ADHD:n eri tautiluokitusten mukaisten diagnostisten kriteerien vertailu»22.
| Keskittymiskyvyttömyys Vähintään 6 oireista on kestänyt vähintään 6 kuukautta, ja oireet ovat haitaksi ja lapsen kehitystasoon nähden poikkeavia. |
|
| Yliaktiivisuus Vähintään 3 oireista on kestänyt vähintään 6 kuukautta, ja oireet ovat haitaksi ja lapsen kehitystasoon nähden poikkeavia. |
|
| Impulsiivisuus Vähintään 3 oireista on kestänyt vähintään 6 kuukautta ja oireet ovat haitaksi ja lapsen kehitystasoon nähden poikkeavia |
|
| Häiriö alkaa viimeistään 7 vuoden iässä. | Diagnostisten kriteerien tulee täyttyä useammassa kuin yhdessä tilanteessa. Esimerkiksi tarkkaamattomuutta ja yliaktiivisuutta tulee esiintyä sekä kotona että koulussa tai sekä koulussa että esimerkiksi vastaanotolla. Tavallisesti tarvitaan tietoa useammasta kuin yhdestä lähteestä. Esimerkiksi opettajan kertomus lapsen käytöksestä on yleensä välttämätön lisä vanhempien kertomuksiin. |
| Oireet aiheuttavat kliinisesti merkittävää ahdistusta tai sosiaalisten, opintoihin liittyvien tai ammatillisten toimintojen heikkenemistä. | |
| Ei ole diagnosoitavissa seuraavia tiloja: maaninen jakso, depressiivinen jakso, ahdistuneisuushäiriö
tai laaja-alaiset kehityshäiriöt. Huom.! Nykykäsityksen mukaan kaikki mainitut häiriöt voivat kuitenkin esiintyä samanaikaisesti ADHD:n kanssa. Diagnoosin kannalta olennaista on, etteivät oireet selity toisella sairaudella. |
Ilmenemismuodot
- ADHD:stä voidaan tunnistaa kolme ilmenemismuotoa sen mukaan, painottuvatko oireet tarkkaamattomuuteen (pääasiassa tarkkaamaton ilmenemismuoto), yliaktiivisuuteen ja impulsiivisuuteen (pääasiassa yliaktiivis-impulsiivinen ilmenemismuoto) vai esiintyykö kaikkia ydinoireita (yhdistetty ilmenemismuoto).
- Suositus 1: Työryhmä suosittaa, että kaikista ilmenemismuodoista käytetään ICD-10-järjestelmässä
diagnoosinumeroa F90.0 Aktiivisuuden ja tarkkaavuuden häiriö ja että ilmenemismuoto
(yhdistetty, tarkkaamaton, yliaktiivis-impulsiivinen) kuvataan tarvittaessa sanallisesti.
Arviointivaiheessa voidaan käyttää diagnoosinumeroa F90.9 tai soveltuvia psykiatrista
tutkimusta (esim. Z00.4) tai yksittäisiä oireita kuvaavia koodeja.
- ICD-10 ohjaa käyttämään pelkästään yliaktiivisuus- ja impulsiivisuuskriteerien täyttyessä diagnoosinumeroa F90.8 (muu määritetty hyperkineettinen häiriö) ja vain tarkkaamattomuuskriteerien täyttyessä diagnoosikoodia F98.8 (muu määritetty tavallisesti lapsuus- tai nuoruusiässä alkava toiminto- ja tunnehäiriö). Koska eri ilmenemismuodoissa ei ole kyse erillisistä häiriöistä, näiden numeroiden käyttö voi lisätä väärinkäsityksiä. Lisäksi F98.8 sisältää muita lapsuusiän häiriöitä, joilla ei ole yhteyttä ADHD:hen.
- Tulevassa ICD-11-järjestelmässä ilmenemismuodot on määritelty selkeämmin kuin käytössä olevassa ICD-10:ssä.
Diagnostiikka
- Suositus 2: ADHD-oireita epäiltäessä tehdään ensin yleinen ja systemaattinen diagnostinen
arvio.
- Arvioon tarvitaan tietoa henkilön nykyisestä ja aiemmasta toimintakyvystä sekä oireiden esiintymisestä erilaisissa tilanteissa, oireiden kestosta sekä oireisiin ja toimintakykyyn vaikuttavista asioista, kuten elämäntilanteesta ja -tavoista «Kooij JJS, Bijlenga D, Salerno L, ym. Updated Euro...»117, «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «AADPA. Australian Evidence-Based Clinical Practice...»124.
- Lisäksi arvioidaan oireiden aiheuttamaa haittaa, muutosta aiemmasta sekä henkilön vahvuuksia ja selviytymisstrategioita.
- Suositus 3: ADHD-oireisiin kohdentuva tarkennettu arviointi aloitetaan, jos kokonaistilanteen
arvion perusteella oirekuva viittaa ADHD:hen, oireet eivät selity elämäntilanteella
tai -tavoilla ja oireista aiheutuu haittaa toimintakyvylle.
- Ks. videot Milloin tarvitaan ADHD-oireiden tarkempaa arviointia? «Milloin tarvitaan ADHD-oireiden tarkempaa arviointia? (video)»2 ja ADHD:n diagnosointi vaatii huolellisen arvion «ADHD:n diagnosointi vaatii huolellisen arvion (video)»3.
- Liian nopea eteneminen ADHD-oireisiin painottuvaan arviointiin lisää diagnostiikan epätarkkuutta ja voi jättää huomioimatta muita tuen tarpeita.
- Väärin perustein tai lievien oireiden perusteella annetusta ADHD-diagnoosista voi olla haittaa ja se voi rajoittaa esimerkiksi ammatinvalintaa, ks. lisätietoa Voiko ADHD-diagnoosista olla lapsille ja nuorille haittaa? «Voiko ADHD-diagnoosista olla lapsille ja nuorille haittaa?»10.
- Systemaattinen ICD- tai DSM-diagnoosikriteereihin perustuva arvio kattaa samanaikaiset
ja erotusdiagnostiset häiriöt (ks. lisätietoa ADHD:n ICD-10-kriteerit «Aktiivisuuden ja tarkkaavuuden (ADHD:n) häiriön kriteerit ICD-10:n mukaan»23), «Kooij JJS, Bijlenga D, Salerno L, ym. Updated Euro...»117, «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «National Guideline Centre (UK). Attention deficit ...»122, «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123, «AADPA. Australian Evidence-Based Clinical Practice...»124.
- Diagnosointi vaatii riittävää ymmärrystä ADHD-oireiden luonteesta sekä kliinistä harkintaa siitä, selittyvätkö vaikeudet ADHD:llä.
- Diagnostinen arvio sisältää esitietojen kartoituksen, ADHD-oireiden määrän, esiintymisen
ja aiheuttaman haitan arvioinnin (haastattelu, tarvittaessa kyselylomakkeet) sekä
lääkärintutkimuksen, ks. tarkempi ohjeisto lisätietoaineistoista Lasten ja nuorten
ADHD-epäily: taustatietokartoitus «Lasten ja nuorten ADHD-epäily: taustatietokartoitus»24 sekä ADHD-diagnoosia varten tehtävä kliininen tutkimus lapsilla ja nuorilla «ADHD-diagnoosia varten tehtävä kliininen tutkimus lapsilla ja nuorilla»25.
- Edellisessä vaiheessa koottuja esitietoja täydennetään tarpeen mukaan, ks. lisätietoa ADHD-oireiden diagnostista arviointia varten koottavia tietoja «ADHD-oireiden diagnostista arviointia varten koottavia tietoja»26.
- Psyykkisen tilan kartoittaminen sisältää sairaushistorian lisäksi samanaikaisten häiriöiden arvioinnin ja mahdollisten muiden keskittymättömyyttä tai levottomuutta provosoivien tekijöiden (esimerkiksi univaje, ahdistus, stressi, elämäntilanne, traumakokemukset) selvittämisen.
- ADHD-oireiden esiintymistä ja haittaavuutta voidaan selvittää haastattelun ja kyselylomakkeiden
avulla.
- Kyselyt tunnistavat herkästi ADHD-oireet, mutta väärien positiivisten mahdollisuus on otettava arvioinnissa huomioon, ks. lisätietoa «Oirekyselyiden ominaisuudet ja rajoitukset ADHD:n diagnostiikassa»27 sekä kohta Oireiden arvioinnin menetelmät «A2»3.
- Usean oireita kartoittavan menetelmän hyödyntäminen lisää arvion osuvuutta. Toisaalta mikään yksittäinen oireita arvioiva menetelmä ei riitä diagnoosin perustaksi, vaan tieto oireista on suhteutettava kokonaisuuteen «Mulraney M, Arrondo G, Musullulu H, ym. Systematic...»119, «Marshall P, Hoelzle J, Nikolas M. Diagnosing Atten...»120.
- Somaattisella tutkimuksella arvioidaan yleinen terveydentila sekä muiden samankaltaisia
oireita aiheuttavien sairauksien mahdollisuus.
- Laboratoriotutkimukset voivat olla tarpeen somaattisia sairauksia epäiltäessä, mutta eivät rutiinimaisesti.
- Kromosomi- tai metabolisia tutkimuksia, EEG:tä tai pään kuvantamistutkimuksia tarvitaan harvoin.
- Erotusdiagnostiikkaa ja kokonaisvaltaista kuntoutussuunnitelmaa varten voidaan oireiden mukaan tarvita myös esimerkiksi puheterapeutin, psykologin, neuropsykologin, toimintaterapeutin tai fysioterapeutin arvio.
- Ympäristö- ja motivaatiotekijät sekä elintapojen merkitys on otettava huomioon oireita arvioitaessa (ks. lisätietoa «ADHD-oireisiin vaikuttavat ympäristö- ja motivaatiotekijät»21).
- Oireita tulee esiintyä useissa erilaisissa tilanteissa.
- Oireiden vähäisyys rauhallisissa kahdenkeskisissä tilanteissa tai kiinnostavan tekemisen aikana ei ole vasta-aihe diagnoosille, jos toimintakykyä haittaavia oireita ilmenee muissa tyypillisissä tilanteissa.
- Elintavoilla, kuten unen, liikunnan ja ruutuajan määrällä ja ruokailujen säännöllisyydellä, on vaikutusta toimintakykyyn ja oireisiin, ks. myös lisätietoa Keskittymisen vaikeuksia, prosessoinnin kuormittumista vai "ADT" aikuisilla? «Keskittymisen vaikeuksia, prosessoinnin kuormittumista vai ”ADT” aikuisilla?»15.
- Suositus 4: Arviointi vaatii yleensä useita tapaamisia ja tiedon hankkimista eri lähteistä.
- Diagnostiikassa keskeistä on asiantuntijan tekemä kliininen haastattelu.
- Oireita tulee esiintyä useassa eri tilanteessa ja eri ihmisten kanssa, joten arviointiin
tarvitaan tietoa toimintakyvystä ja oireiden haittaavuudesta kotona, koulussa (tunneilla,
välitunnilla), opiskelupaikassa tai työpaikassa.
- Lasten ja nuorten oireiden arviointiin kuuluu sekä lapsen että hänen huoltajiensa tapaaminen «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «AADPA. Australian Evidence-Based Clinical Practice...»124.
- Myös aikuisten oireiden arvioimisessa on hyötyä läheisen (puoliso, vanhemmat, sisarukset) antamista tiedoista.
- Diagnostisen tutkimuksen tukena voidaan käyttää diagnostista kaaviota «ADHD:n diagnostinen kaavio»1 ja diagnosoinnin muistilistaa «ADHD:n diagnostisen arvion muistilista»28.
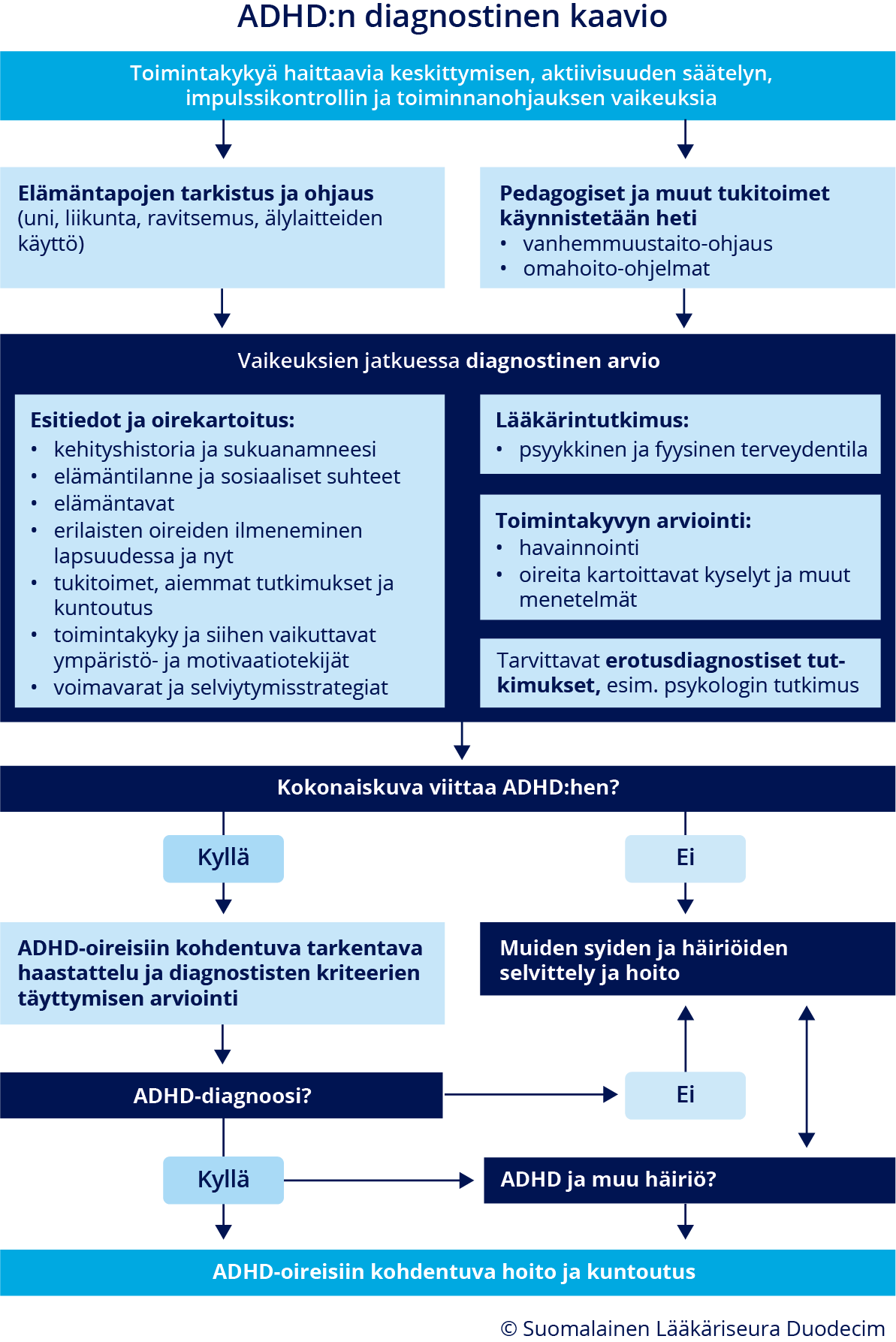
ADHD:n diagnostinen kaavio.
Diagnosointi eri ikävaiheissa
- Lapsilla ja nuorilla aktiivisuuden ja tarkkaavuuden häiriö on otettava huomioon yhtenä vaihtoehtona, kun
esiintyy koulunkäyntiin tai käyttäytymiseen liittyviä ongelmia tai ahdistuneisuusoireita,
joista vanhemmilla, varhaiskasvatuksen, koulun tai opiskelupaikan henkilökunnalla
tai nuorella itsellään on huolta «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «Eom TH, Kim YH. Clinical practice guidelines for a...»121.
- Tyypilliset ADHD-oireet ovat usein havaittavissa jo leikki-iässä, mutta diagnoosin tekeminen ennen kouluikää vaatii erityistä huolellisuutta (ks. lisätietoa «ADHD:n tunnistaminen ja diagnosointi ennen kouluikää»29). Luotettava diagnosoiminen ei oireiden epäspesifisyyden vuoksi useinkaan ole mahdollista ennen 5 vuoden ikää «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «Eom TH, Kim YH. Clinical practice guidelines for a...»121.
- Lapsen toimintakykyä sekä tarkkaavuus-, yliaktiivisuus- ja impulsiivisuusoireita pitää arvioida suhteessa ikä- ja kehitystasoon, ja niiden esiintymisestä tarvitaan useiden ihmisten (vanhemmat, opettajat) havaintoja eri tilanteista (kotona, varhaiskasvatuksessa tai koulussa, harrastuksissa tms.) «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «National Guideline Centre (UK). Attention deficit ...»122. Myös lapsen omaa arviota oireista ja niiden aiheuttamasta haitasta on kysyttävä.
- Perhe- ja koulutilanteeseen ja ihmissuhteisiin liittyvät mahdolliset stressitekijät
tulee selvittää.
- Erityistä huomiota kannattaa kiinnittää sosiaalihuoltolain mukaisia tukitoimia tarvitseviin, erityisesti sijoitettujen lasten ja nuorten psyykkisen tilanteen arviointiin «AADPA. Australian Evidence-Based Clinical Practice...»124, «Penttilä S, Niemelä M, Hakko H, ym. Child- and par...»125.
- Maahanmuuttajien lapsilla voi olla tavallista suurempi ADHD-oireiden riski, mutta myös muita oireita selittäviä syitä «Lehti V, Chudal R, Suominen A, ym. Association bet...»126.
- Epäily aikuisen ADHD:stä voi herätä henkilöllä itsellään, hänen läheisillään, työpaikalla tai perusterveydenhuollossa,
esimerkiksi opiskelu- tai työterveyshuollossa. Myös lapsella todettu ADHD voi johtaa
tarpeeseen arvioida vanhemman ADHD-oireita. ADHD:n mahdollisuus tulee ottaa huomioon
kaikkien mielenterveyshäiriöiden yhteydessä (etenkin itsetuhoisuuden, päihdehäiriöiden,
persoonallisuushäiriöiden, psykoosien, syömishäiriöiden ja internet- tai peliriippuvuuden
yhteydessä), etenkin jos asianmukainen hoito ei ole lievittänyt oireita.
- ADHD:n oirekuva muuttuu usein iän myötä, ja aikuisiin kohdentuvat ulkoiset vaatimukset vaikuttavat oireiden aiheuttamaan haittaan. DSM-5-diagnoosiluokituksessa tämä on otettu huomioon siten, että 17-vuotiailla ja sitä vanhemmilla ADHD-diagnoosiin riittää yhteensä 5 tarkkaamattomuus- tai yliaktiivisuus-impulsiivisuusoiretta (ks. lisätietoa «ADHD:n eri tautiluokitusten mukaisten diagnostisten kriteerien vertailu»22).
- Aikuinen on omien oireidensa ja niiden aiheuttaman haitan tärkein tiedonlähde.
- Oiretiedostus saattaa kuitenkin aikuisillakin vaihdella, ja aikuinen saattaa ylikorostaa tai aliarvioida oireitaan. Läheisen, esimerkiksi puolison, vanhemman tai sisaruksen, antama tieto saattaa auttaa oireiden aiheuttaman toiminnallisen haitan arvioinnissa.
- Muistikuvat lapsuudesta eivät välttämättä ole luotettavia.
- Lisätietoa oireiden esiintymisestä voi saada aiemmista terveys- ja sairauskertomusmerkinnöistä
tai esimerkiksi koulutodistusten sanallisista kuvauksista ja oppimisen tuen suunnitelmista.
Nämä tiedot on suhteutettava kyseisen ajankohdan käytäntöihin, esimerkiksi kouluarvosanojen
kriteereihin tai oppimisen tuen tarjolla olleisiin menetelmiin.
- Näin saatava tieto voi tukea diagnostista arviota, mutta oireiden puuttuminen lapsuusiän
objektiivisista dokumenteista ei sulje pois ADHD:n mahdollisuutta.
- Tarkkaamattomuusoireet eivät välttämättä aiheuta merkittävää haittaa ennen toisen asteen opintoja, jotka vaativat enemmän organisointikykyä ja itsenäistä työskentelyä «AADPA. Australian Evidence-Based Clinical Practice...»124.
- Lapsuus- tai nuoruusiän toimintakyvystä kertovia lähteitä ei aina ole käytettävissä, mikä ei saa estää diagnostisen arvion tekemistä «Marshall P, Hoelzle J, Nikolas M. Diagnosing Atten...»120.
- Näin saatava tieto voi tukea diagnostista arviota, mutta oireiden puuttuminen lapsuusiän
objektiivisista dokumenteista ei sulje pois ADHD:n mahdollisuutta.
- Jos aikuiselle on tehty ADHD-diagnoosi lapsuus- tai nuoruusiässä, mutta sen hoitoon
tai seurantaan on tullut taukoa, arvioidaan
- ajankohtainen oirekuva ja oireiden aiheuttama haitta
- muut mahdolliset oireita vaikeuttavat psykiatriset sairaudet (yleisimpinä mieliala-, ahdistuneisuus- tai päihdehäiriöt) ja niiden vaikutus toimintakykyyn.
- Jos ADHD-diagnoosia ei ole tehty lapsuus- tai nuoruusiässä, on selvitettävä, kuinka
kauan oireet ovat kestäneet.
- Joidenkin tutkimusten perusteella on esitetty, että ADHD voisi alkaa vasta aikuisiällä «Caye A, Rocha TB, Anselmi L, ym. Attention-Deficit...»127, «Agnew-Blais JC, Polanczyk GV, Danese A, ym. Evalua...»128, «Moffitt TE, Houts R, Asherson P, ym. Is Adult ADHD...»129. Nykyisten ja tulevienkin ICD-järjestelmän diagnostisten määritelmien mukaan diagnoosin edellytyksenä on kuitenkin oireiden alkaminen lapsuudessa (ennen 12 vuoden ikää) «The World Health Organization (WHO). International...»130.
- Kaikkien diagnoosikriteerien täyttymistä lapsuusiässä ei tarvitse osoittaa. Riittää, että potilaalla tiedetään viimeistään alakouluiässä esiintyneen useita ADHD-oireita.
- Lapsuudenaikaisia oireita selvitettäessä on otettava huomioon myös vanhempien antama tavanomaisesta poikkeava tuki ja esimerkiksi koulussa toteutetut tukitoimet. Riittävät tukitoimet parantavat toimintakykyä, esimerkiksi koulusuoriutumista. Siksi pelkästään suoriutumisen arviointi ei riitä.
Oireiden arvioinnin menetelmät
- Esitietojen täydentämisessä ja oireiden esiintymisen, määrän ja haittaavuuden arvioimisessa
voidaan käyttää oirekyselyitä tai muita oirekartoituksen menetelmiä osana kokonaisarviota,
ks. myös suositukset 2 ja 3 «A3»4.
- Mikään näistä menetelmistä ei ainoana arvioinnin keinona ole riittävä «Mulraney M, Arrondo G, Musullulu H, ym. Systematic...»119, «Marshall P, Hoelzle J, Nikolas M. Diagnosing Atten...»120, «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «National Guideline Centre (UK). Attention deficit ...»122, «Peterson BS, Trampush J, Brown M, ym. Tools for th...»131, «Harrison AG, Edwards MJ. The Ability of Self-Repor...»132, «Arrondo G, Mulraney M, Iturmendi-Sabater I, ym. Sy...»133, ks. lisätietoa «Oirekyselyiden ominaisuudet ja rajoitukset ADHD:n diagnostiikassa»27.
- Suositus 5: Erilaisia oirearviointimenetelmiä tulee käyttää vain osana laajaa kokonaisarvioita.
Ne tunnistavat ADHD-oireita herkästi, mutta voivat tuottaa vääriä positiivisia tuloksia
riittämättömän tarkkuuden vuoksi «Mulraney M, Arrondo G, Musullulu H, ym. Systematic...»119, «Marshall P, Hoelzle J, Nikolas M. Diagnosing Atten...»120, «Caselles-Pina L, Quesada-López A, Sújar A, ym. A s...»134, «Sawaya H, Miller JC, Raines JM. Review of Studies ...»135.
- Se, miten kyselyyn vastaaja ymmärtää kyselyn väittämät ja pystyy arvioimaan oireiden asiayhteyttä, voi vaikuttaa kyselyvastausten luotettavuuteen (voi aiheuttaa sekä oireiden liiallista että liian vähäistä tunnistamista) «Mulraney M, Arrondo G, Musullulu H, ym. Systematic...»119.
- Suositus 6: Oirekyselyn pisterajan ylittävää tulosta suositellaan tarkennettavaksi haastattelulla, jossa pyydetään esimerkiksi omasanaisia esimerkkejä ongelmista ja niiden aiheuttamasta haitasta, oireiden alkamisiästä ja kestosta sekä tilanteista, jossa oireet ilmenevät.
- Oireiden kartoituksessa voidaan käyttää laajemmin psyykkistä toimintakykyä ja oirekuvaa
kartoittavia tai kapeammin ADHD-oireisiin kyselyitä.
- Laaja-alaiset oirekyselyt ja puolistrukturoidut haastattelut (esimerkiksi lapsilla ja nuorilla SDQ, DAWBA, CBCL, K-SADS-PL 2013 ja Young Diva 5, aikuisilla DIVA 2.0 ja ACE+) arvioivat laajasti käyttäytymisen piirteitä ja psyykkistä toimintakykyä, myös ADHD-oireita, ks. lisätietoa «Laaja-alaiset oirekartoitusmenetelmät lasten ADHD-oireiden arvioinnissa»30 ja «Aikuisten ADHD-kyselylomakkeet ja puolistrukturoidut haastattelut»31.
- ADHD-oireisiin kohdentuvia kyselyitä ovat esimerkiksi
- ADHD-oirelomake «hoi50061d.pdf»1
- ADHD Rating Scale IV (ADHD-RS-IV) «hoi50061g.pdf»2 (ks. lisätietoa «ADHD Rating Scale IV -kyselylomakkeen käyttäminen»32), saameksi «hoi50061h.pdf»3, «hoi50061i.pdf»4, «hoi50061j.pdf»5
- lapsilla lisäksi Keskittymiskysely (Kesky), PikkuKesky ja Five to Fifteen (FTF) eli Viivi-kysely, (ks. lisätietoa «Lasten ADHD-oireisiin kohdennetut oirekyselyt»33)
- aikuisilla lisäksi esimerkiksi ASRS ja Five to Fifteen (FTF) eli Viivi-kyselyä voidaan käyttää myös aikuisten lapsuudenaikaisten neurokehityksellisten oireiden takautuvaan arvioimiseen, (ks. lisätietoa «Aikuisten ADHD-kyselylomakkeet ja puolistrukturoidut haastattelut»31).
- Diagnostiikan avuksi on kehitetty myös reaktioita, suoritus- tai toimintakykyä arvioivia
tietokoneistettuja arviointimenetelmiä, ks. lisätietoa ADHD-oireiden arvioinnin muut menetelmät «ADHD-oireiden arvioinnin muut menetelmät»34.
- Näiden menetelmien soveltuvuutta ADHD:n arvioimiseen on tutkittu toistaiseksi niukasti, eikä niiden tarkkuudesta tai herkkyydestä ADHD-oireiden arvioinnissa ole luotettavaa tietoa.
- Menetelmien tulosten tulkinta kuuluu käytetyn testin hyvin tuntevalle diagnostiikan ammattilaiselle.
Neuropsykologinen tutkimus
- Neuropsykologisella (tai neuropsykologisesti orientoituneella psykologisella, neuropsykologin
ohjauksessa tehdyllä) tutkimuksella (ks. lisätietoa «Neuropsykologinen tutkimus ja ADHD»35) saadaan kuntoutuksen ja tukitoimien suunnittelun kannalta tärkeää lisätietoa kognitiivisista
taidoista ja samanaikaisista ongelmista, kuten oppimisvaikeuksista sekä niiden vaikutuksista opiskelussa ja työssä suoriutumiseen. Tutkimus ei kuitenkaan ole välttämätön ADHD-oireiden arvioimiseksi eikä diagnoosin
tekemistä varten.
- Pelkästään kognitiivisten testien perusteella ADHD-diagnoosia ei voida tehdä, sillä
niiden tulokset eivät ole yksilötasolla erottelevia «Sadozai AK, Sun C, Demetriou EA, ym. Executive fun...»113, «Korkeila J, Leppämäki S, Virta M. Aktiivisuuden ja...»136. Neuropsykologisessa tutkimuksessa ei ole aina todettavissa vaikeuksia, vaikka henkilöllä
olisi diagnosoitavissa ADHD.
- Suoriutuminen saattaa jäsennetyssä testaustilanteessa olla selvästi parempaa kuin luonnollisissa tilanteissa. Tutkimuksen tulee olla laaja. Tiedon hankkiminen toimintakyvystä eri tilanteissa haastatteluilla tai kyselylomakkeilla on olennainen osa psykologista arviointia.
- Neuropsykologinen (tai neuropsykologisesti orientoitunut psykologinen) tutkimus tulee tehdä aina, kun harkitaan neuropsykologisen kuntoutuksen tarvetta «Neuropsykologinen kuntoutus ja ADHD»36.
- Pelkästään kognitiivisten testien perusteella ADHD-diagnoosia ei voida tehdä, sillä
niiden tulokset eivät ole yksilötasolla erottelevia «Sadozai AK, Sun C, Demetriou EA, ym. Executive fun...»113, «Korkeila J, Leppämäki S, Virta M. Aktiivisuuden ja...»136. Neuropsykologisessa tutkimuksessa ei ole aina todettavissa vaikeuksia, vaikka henkilöllä
olisi diagnosoitavissa ADHD.
Erotusdiagnostiikassa huomioitavat sairaudet ja häiriöt
- Suositus 7: ADHD:n diagnostiikassa on arvioitava, selittyvätkö oireet muilla sairauksilla
tai häiriöillä tai niiden hoitoon käytettyjen lääkkeiden haittavaikutuksilla.
- Monet erotusdiagnostisesti olennaisista häiriöistä voivat esiintyä myös samanaikaisesti
ADHD:n kanssa. Ks. kohta Hoito ADHD:n kanssa samanaikaisesti esiintyvien häiriöiden
ja sairauksien yhteydessä «A6»5.
- Komplisoituneen ADHD:n arvioinnin ja hoidon algoritmeja esitellään artikkelissa «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123
- Muun häiriön diagnoosi ei estä ADHD-diagnoosin käyttöä, jos molempien häiriöiden diagnostiset kriteerit täyttyvät.
- Tarpeelliset erotusdiagnostiset tutkimukset valitaan esitietojen ja lääkärintutkimuksen perusteella.
- Monet erotusdiagnostisesti olennaisista häiriöistä voivat esiintyä myös samanaikaisesti
ADHD:n kanssa. Ks. kohta Hoito ADHD:n kanssa samanaikaisesti esiintyvien häiriöiden
ja sairauksien yhteydessä «A6»5.
- Erotusdiagnostiikassa huomioitavia sairauksia ja häiriöitä ovat esimerkiksi
- somaattiset ja neurologiset sairaudet, jotka voivat aiheuttaa samankaltaisia oireita
- aistisairaudet (näkö, kuulo)
- unen häiriöitä aiheuttavat sairaudet (kuten uniapnea ja levottomat jalat)
- aineenvaihduntasairaudet (esimerkiksi diabetes, kilpirauhasen toimintahäiriöt)
- anemia
- keliakia
- muistisairaudet
- poissaolokohtauksina esiintyvä epilepsia «Epilepsia ADHD:n samanaikaissairautena ja erotusdiagnostiikassa»37
- aivovammat ja niiden jälkitilat (ks. Käypä hoito -suositus Aivovammat «Aivovammat»6, «Aivovammat. Suomalaisen Lääkäriseuran Duodecimin, ...»137)
- kehitykselliset häiriöt
- oppimisvaikeudet (mm. lukemisen ja kirjoittamisen erityisvaikeus), myös aikuisilla «Oppimisvaikeudet ja ADHD»38
- kehityksellinen kielihäiriö (kielellinen erityisvaikeus) (ks. Käypä hoito -suositus Kehityksellinen kielihäiriö (kielellinen erityisvaikeus, lapset ja nuoret) «Kehityksellinen kielihäiriö (kielellinen erityisvaikeus, lapset ja nuoret)»7, «Kehityksellinen kielihäiriö (kielen kehityksen häi...»138)
- kehityksellinen koordinaatiohäiriö (ks. Käypä hoito -suositus Lasten ja nuorten kehityksellinen koordinaatiohäiriö (DCD) «Lasten ja nuorten kehityksellinen koordinaatiohäiriö (DCD)»8, «Lasten ja nuorten kehityksellinen koordinaatiohäir...»139)
- monimuotoiset kehityshäiriöt, laaja-alaiset oppimisvaikeudet ja kehitysvammaisuus
- autismikirjon häiriö (ks. Käypä hoito -suositus Autismikirjon häiriö «Autismikirjon häiriö»9, «Autismikirjon häiriö. Käypä hoito -suositus. Suoma...»140)
- psyykkiset sairaudet ja häiriöt
- käytöshäiriöt (ks. Käypä hoito -suositus Käytöshäiriöt (lapset ja nuoret) «Käytöshäiriöt (lapset ja nuoret)»10, «Käytöshäiriöt (lapset ja nuoret). Käypä hoito -suo...»141, ja lisätietoa «Käytöshäiriöt ja ADHD»39)
- kiintymyssuhdehäiriö «Lapsuuden kiintymyssuhdehäiriöt ja ADHD»40
- ahdistuneisuushäiriöt (ks. Käypä hoito -suositus Ahdistuneisuushäiriöt «Ahdistuneisuushäiriöt»11, «Ahdistuneisuushäiriöt. Käypä hoito -suositus. Suom...»142) ja pakko-oireinen häiriö (ks. Käypä hoito -suositus Pakko-oireinen häiriö (OCD) «Pakko-oireinen häiriö (OCD)»12, «Pakko-oireinen häiriö. Käypä hoito -suositus. Suom...»143)
- mielialahäiriöt: masennus (ks. Käypä hoito -suositus Depressio «Depressio»13, «Depressio. Käypä hoito -suositus. Suomalaisen Lääk...»144) ja kaksisuuntainen mielialahäiriö (ks. Käypä hoito -suositus Kaksisuuntainen mielialahäiriö «Kaksisuuntainen mielialahäiriö»14, «Kaksisuuntainen mielialahäiriö. Käypä hoito -suosi...»145, sekä lisätietoa «ADHD ja kaksisuuntainen mielialahäiriö lapsuudessa ja nuoruudessa»41)
- traumaperäinen stressihäiriö (ks. Käypä hoito -suositus Traumaperäinen stressihäiriö «Traumaperäinen stressihäiriö»15, «Traumaperäinen stressihäiriö. Käypä hoito -suositu...»146, ja lisätietoa «ADHD ja traumaperäiset häiriöt»42)
- epävakaa persoonallisuushäiriö (ks. Käypä hoito -suositus Epävakaa persoonallisuus «Epävakaa persoonallisuus»16, «Epävakaa persoonallisuus. Käypä hoito -suositus. S...»147)
- päihdehäiriöt ja toiminnalliset riippuvuudet (ks. Käypä hoito -suositukset Alkoholiongelmat «Alkoholiongelmat»17, «Alkoholiongelmat. Käypä hoito -suositus. Suomalais...»148, Huumeongelmat «Huumeongelmat»18, «Huumeongelmat. Käypä hoito -suositus. Suomalaisen ...»149 ja Rahapeliongelma «Rahapeliongelma»5, «Rahapeliongelma. Käypä hoito -suositus. Suomalaise...»106, «Findon JL, Muck A, Tóthpál-Davison B, ym. Investig...»105).
- psykoottiset häiriöt (ks. Käypä hoito -suositus Skitsofrenia «Skitsofrenia»19, «Skitsofrenia. Käypä hoito -suositus. Suomalaisen L...»150 ja lisätietoa «ADHD ja psykoottiset oireet lapsilla ja nuorilla»43)
- somaattiset ja neurologiset sairaudet, jotka voivat aiheuttaa samankaltaisia oireita
- Lisätietoaineistossa Erotusdiagnostiikkataulukko «Erotusdiagnostiikka ADHD:ssä (ADHD, depressio, kaksisuuntainen mielialahäiriö, ahdistuneisuushäiriö ja traumaperäinen stressihäiriö)»44 vertaillaan ADHD:n, masennuksen, kaksisuuntaisen mielialahäiriön, ahdistuneisuuden ja traumaperäisen stressihäiriön oirekuvia.
Hoito ja kuntoutus
Hoidon yleiset periaatteet
- Hoito on monimuotoista, ja siihen kuuluvat aina tiedollinen ohjaus ja neuvonta (psykoedukaatio)
sekä erilaiset tarpeellisiksi arvioidut yksilölliset tukitoimet ja hoitomuodot «Kooij JJS, Bijlenga D, Salerno L, ym. Updated Euro...»117, «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123 «AADPA. Australian Evidence-Based Clinical Practice...»124, «Wolraich ML, Hagan JF Jr, Allan C, ym. Clinical Pr...»151, «Mechler K, Banaschewski T, Hohmann S, ym. Evidence...»152, «Chan E, Fogler JM, Hammerness PG. Treatment of Att...»153, «Torgersen T, Gjervan B, Lensing MB, ym. Optimal ma...»154, «Sibley MH, Flores S, Murphy M, ym. Research Review...»155.
- Ks. vuokaavio hoidosta «ADHD:n hoito ja kuntoutus»2.
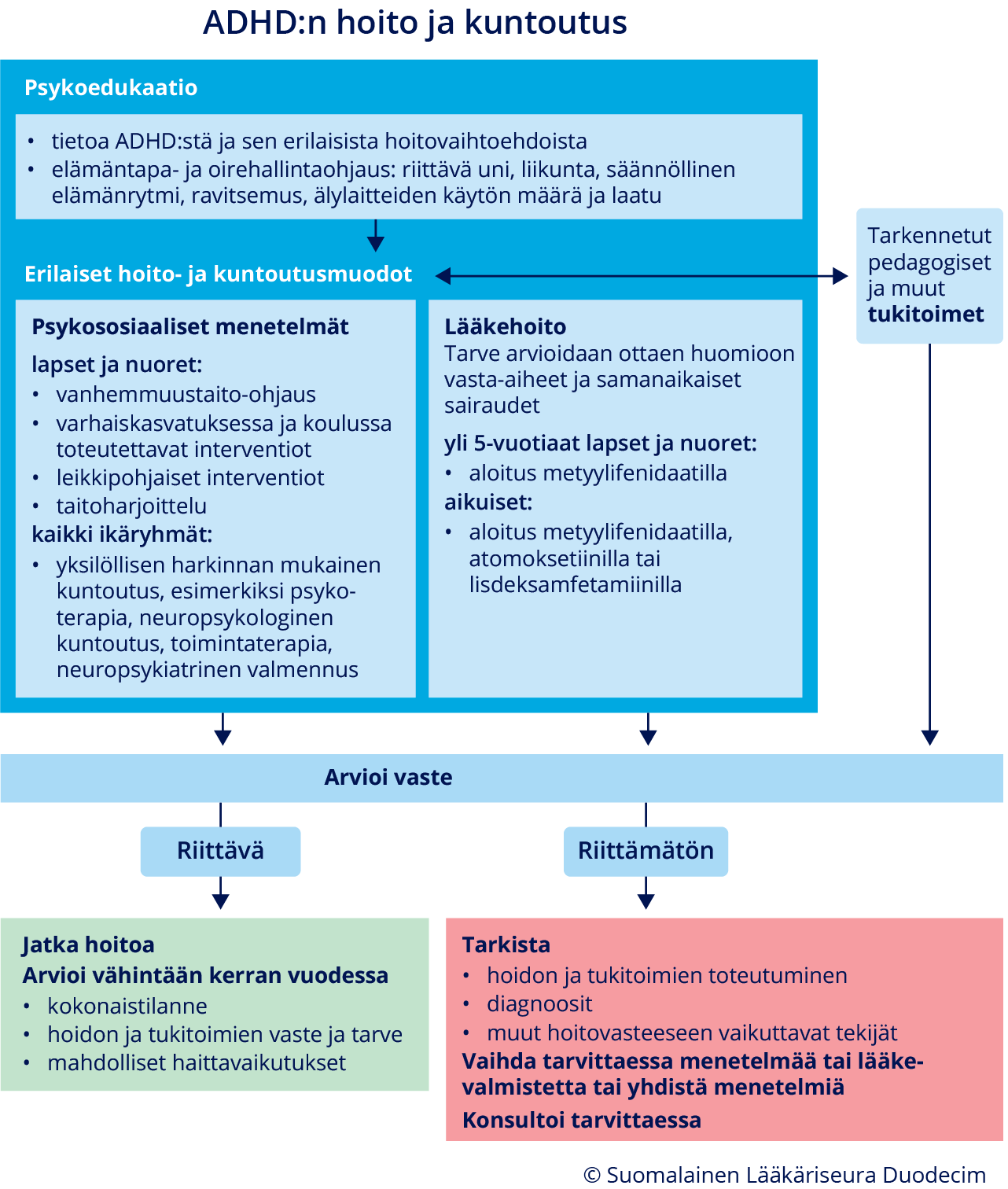
ADHD:n hoito ja kuntoutus.
- Suositus 8: Tukitoimet aloitetaan heti, kun havaitaan tarkkaavuuteen, yliaktiivisuuteen
tai impulsiivisuuteen liittyviä toiminta- tai oppimiskyvyn ongelmia. Jos tukitoimet
lievittävät oireita riittävästi, tarkempia tutkimuksia ADHD:n arvioimiseksi ei välttämättä
tarvita.
- Tukitoimien aloittaminen ei vaadi diagnoosia.
- Keskeisiä periaatteita ovat käyttäytymisen ohjaamisen ja haittaavien oireiden hallinnan menetelmät sekä ympäristön muokkaaminen toimintakykyä tukevaksi.
- Ks. video Tukitoimet aloitetaan heti huolen herätessä «Tukitoimet aloitetaan heti huolen herätessä (video)»1.
- Toimintakykyä tukevia keinoja ovat esimerkiksi
- vanhemmille suunnattu ohjaus ja neuvonta (perheneuvonta)
- varhaiskasvatuksessa, koulussa ja opiskelussa tarvittavat pedagogiset toimet ja muut toimintakykyä tukevat järjestelyt
- psykologin, neuropsykologin tai puhe-, toiminta- tai fysioterapeutin arvion perusteella annettava ohjaus tai kuntoutus
- mielenterveystalon omahoito-ohjelmat vanhemmille, nuorille ja aikuisille «https://www.mielenterveystalo.fi»2
- sosiaalihuoltolain mukaiset tukimuodot, esimerkiksi tukihenkilö tai -perhe ja perhetyö.
- Suositus 9: Erityistä huomiota tulee kiinnittää yleisesti hyvinvointiin vaikuttaviin elintapoihin (uni, liikunta, päivärytmi, ravitsemus ja sähköisen median käyttö).
- Suositus 10: Diagnoosin varmistuttua potilaalle ja hänen läheisilleen pitää antaa
tietoa ADHD:stä sekä ohjausta oireiden hallintaa ja arjen sujuvuutta lisäävistä keinoista
ja erilaisista hoitomuodoista «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123, «AADPA. Australian Evidence-Based Clinical Practice...»124, «Wolraich ML, Hagan JF Jr, Allan C, ym. Clinical Pr...»151.
- Neuvonnan välineinä voidaan käyttää erilaisia esitteitä ja videoita sekä verkkosivustoja,
esimerkiksi Mielenterveystalon materiaaleja ja omahoito-ohjelmia.
- Vanhemmille annettavat ohjeet ADHD-oireisen lapsen tai nuoren ohjaamisesta (ks. lisätietoa «Vanhemmille annettavat ohjeet ADHD-oireisen lapsen tai nuoren ohjaamisesta»45 sekä ADHD-liiton julkaisema opas Arki toimimaan «https://adhd-liitto.fi/adhd-julkaisut/arki-toimimaan-vinkkeja-lapsen-myonteiseen-tukemiseen/»3)
- Aikuiselle tai nuorelle annettavat ohjeet (ks. lisätietoa Keinoja arjen hallinnan parantamiseksi «Keinoja aikuisille ja nuorille arjen hallinnan parantamiseksi ja ADHD-oireiden hallitsemiseksi»46 sekä ADHD-liiton julkaisema opas Aikuisen arki toimimaan «https://adhd-liitto.fi/adhd-julkaisut/aikuisen-arki-toimimaan/»4)
- Konkreettinen ohjaus/valmennus arkiympäristössä koetaan usein hyödylliseksi.
- Ryhmämuotoista psykoedukaatiota voi saada esimerkiksi ensitietopäiviltä ja sopeutumisvalmennuskursseilta, jotka tarjoavat myös vertaistukea (ks. lisätietoa «ADHD ja vertaistuki»47).
- Vuonna 2020 tehdyn meta-analyysin mukaan vanhemmille annettu psykoedukaatio lievittää lasten ADHD- ja käytösoireita, lisää ymmärrystä ADHD:n vaikutuksista ja tukee hoitoon sitoutumista «Dahl V, Spears AP, ym. Psychoeducation interventio...»156.
- Neuvonnan välineinä voidaan käyttää erilaisia esitteitä ja videoita sekä verkkosivustoja,
esimerkiksi Mielenterveystalon materiaaleja ja omahoito-ohjelmia.
- Suositus 11: ADHD-oireita voidaan hoitaa sekä psykososiaalisilla hoitomuodoilla että
lääkehoidolla «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123, «AADPA. Australian Evidence-Based Clinical Practice...»124, «Wolraich ML, Hagan JF Jr, Allan C, ym. Clinical Pr...»151, «Mechler K, Banaschewski T, Hohmann S, ym. Evidence...»152, «Chan E, Fogler JM, Hammerness PG. Treatment of Att...»153, «Sibley MH, Flores S, Murphy M, ym. Research Review...»155, «Brown RT, Amler RW, Freeman WS, ym. Treatment of a...»157 «Vidal-Estrada R, Bosch-Munso R, Nogueira-Morais M,...»158, «Young S, Khondoker M, Emilsson B, ym. Cognitive-be...»159, «Philipsen A, Jans T, Graf E, ym. Effects of Group ...»160. Hoidon tarve ja kuntoutuksen menetelmät arvioidaan yksilöllisesti.
- ADHD-diagnoosin saaneet eivät tarvitse rutiinimaisesti kaikkia hoitoja, vaan eri hoitomuotojen
tarve ja järjestys tulee arvioida yksilöllisesti.
- Ks. video ADHD:n hyvä hoito vastaa yksilöllisiin tarpeisiin «ADHD:n hyvä hoito vastaa yksilöllisiin tarpeisiin (video)»4.
- Usean hoitomuodon (erilaisten psykososiaalisten hoitojen tai psykososiaalisten hoitomuotojen ja lääkehoidon) yhdistäminen ja samanaikainen toteuttaminen on tavallista ja usein tarpeellista.
- Hoito ja kuntoutus kohdennetaan iän ja kehitysvaiheen mukaisella tavalla «Young S, Amarasinghe JM. Practitioner review: Non-...»161, (ks. lisätietoa «ADHD-hoidon menetelmien valinta eri ikävaiheissa»48).
- Lasten ja nuorten kuntoutus tulee suunnitella ja toteuttaa yhteistyössä vanhempien ja lapsen tai nuoren kanssa ikä ja kehitystaso huomioiden.
- Kuntoutukseen ohjaamisessa noudatetaan valtakunnallisia lääkinnälliseen kuntoutukseen ohjaamisen perusteita «https://julkaisut.valtioneuvosto.fi/handle/10024/164488»5, «Sosiaali- ja terveysministeriö. Valtakunnalliset l...»162.
- ADHD-diagnoosin saaneet eivät tarvitse rutiinimaisesti kaikkia hoitoja, vaan eri hoitomuotojen
tarve ja järjestys tulee arvioida yksilöllisesti.
- Suositus 12: Hoito- ja kuntoutussuunnitelmaan kirjataan suunnitellut tukitoimet, hoito ja kuntoutus sekä asetetut hoitotavoitteet, eri toimijoiden välinen työnjako, seurannasta vastaava yksikkö ja aikataulu.
- Samanaikaisten sairauksien hoidon tarve ja hoitojärjestys tulee arvioida kokonaisuutena
«Eom TH, Kim YH. Clinical practice guidelines for a...»121, «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123.
- Kuntoutussuunnitelmaa laadittaessa huomioidaan myös henkilön vahvuudet, joita voidaan hyödyntää kuntoutuksen toteutuksessa.
- Hoidon alkaessa määritetään hoidon tavoitteet (esim. levottomuuden väheneminen, läksyjen
teon onnistuminen, työtehtävään keskittymisen parantuminen), joiden saavuttamista
hoidon aikana arvioidaan. Hoidon ja sen seurannan on oltava pitkäjänteistä «Riddle MA, Yershova K, Lazzaretto D, ym. The Presc...»163, «Vitiello B, Lazzaretto D, Yershova K, ym. Pharmaco...»164.
- Tavoitteiden asettamisessa ja hoidon vaikuttavuuden arvioinnissa voidaan käyttää esimerkiksi
ICF-luokittelua (International Classification of Functioning, Disability and Health)
«https://thl.fi/aiheet/toimintakyky/icf-luokitus»6.
- ICF-luokitus kuvaa toimintakykyä, ks. lisätietoa «ICF-luokitus toimintakyvyn ja ADHD-oireiden kuvaamisessa»49. Erilaisiin terveydentiloihin ja tilanteisiin soveltuvista koodeista on laadittu ydinlistoja, jollainen on myös ADHD:stä «Bölte S, Mahdi S, Coghill D, ym. Standardised asse...»165, «Bölte S, Alehagen L, Black MH, ym. Assessment of f...»166, «de Schipper E, Lundequist A, Wilteus AL, ym. A com...»167.
- Hoidon tehoa, tavoitteiden saavuttamista sekä ADHD-oireiden määrää ja haittaavuutta seurataan haastattelun, kliinisen arvion ja tarvittaessa kyselylomakkeiden (esim. ADHD-oirelomake «hoi50061d.pdf»1 tai lääkehoidon seurantalomake «hoi50061c.pdf»6) avulla.
- Hoitomyöntyvyydellä ja hoidon koetulla hyväksyttävyydellä on vaikutusta hoidon toteutumiseen ja siten myös tehoon (ks. lisätietoa «ADHD:n hoitovasteeseen ja hoitoon sitoutumiseen vaikuttavat tekijät»50).
- Tavoitteiden asettamisessa ja hoidon vaikuttavuuden arvioinnissa voidaan käyttää esimerkiksi
ICF-luokittelua (International Classification of Functioning, Disability and Health)
«https://thl.fi/aiheet/toimintakyky/icf-luokitus»6.
- ADHD tai sen vaikutukset toimintakykyyn voivat tuoda oikeuden Kelan etuuksiin, ks.
Suomen Lääkärilehden artikkeli «Puustjärvi A, Kallio-Laine K, Klintrup K ym. Tunne...»168 ja lisätietomateriaali Kelan etuudet «Kelan etuudet ADHD:tä sairastavalle potilaalle. Päivitetty 25.6.2026»51.
- Yleisin ADHD:n perusteella haettu Kelan etuus on lääkekorvausoikeus.
- Lasten tavallisimmat etuudet ovat alle 16-vuotiaan vammaistuki ja erilaiset vaativana lääkinnällisenä kuntoutuksena myönnetyt kuntoutusmuodot.
- Nuorten tavallisimpia etuuksia ovat erilaiset opiskelu- ja työelämävalmiuksia tukevat kuntoutusmuodot.
- Aikuisten ADHD ainoana häiriönä oikeuttaa harvoin Kelan työ- ja toimintakykyetuuksiin.
Perheen tukeminen osana hoitoa
- Perinnöllisten tekijöiden vuoksi on tavallista, että samassa perheessä sekä vanhemmalla
että lapsella on ADHD «Uchida M, Driscoll H, DiSalvo M, ym. Assessing the...»169.
- Vanhemman ADHD voi vaikeuttaa arjen rakenteiden ylläpitoa, kasvatuksen johdonmukaisuutta ja vanhemman kykyä tukea lapsen tunteiden ja käytöksen säätelytaitojen kehittymistä «Theule J, Wiener J. Parenting Stress in Families o...»170, «Endo K, Stanyon D, Yamasaki S, ym. Self-Reported M...»171. Se voi myös heikentää kykyä hyötyä vanhemmuustaito-ohjauksesta ja toteuttaa esimerkiksi käyttäytymishoidollisia menetelmiä «Johnston C, Mash EJ, Miller N, ym. Parenting in ad...»172, «Friedman LM, Dvorsky MR, McBurnett K, ym. Do Paren...»173
- ADHD suurentaa myös parisuhdeongelmien riskiä «Wymbs BT, Canu WH, Sacchetti GM, ym. Adult ADHD an...»174.
- Suositus 13: Vanhempien ADHD:n hyvä hoito on tärkeää ylisukupolvisten vaikeuksien
minimoimiseksi. Perheenjäsenten, esimerkiksi vanhemman ja lapsen, hoitojen synkronointi
voi olla hyödyllistä «Webster-Stratton CH, Reid MJ, Beauchaine T. Combin...»175, «Chronis-Tuscano A, Wang CH, Woods KE, ym. Parent A...»176, «Friedman LM, Dvorsky MR, McBurnett K, ym. Do Paren...»173.
- Vanhempien mahdollisia muitakin psyykkisiä häiriöitä (esim. masennus) tulee hoitaa tehokkaasti «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «AADPA. Australian Evidence-Based Clinical Practice...»124.
- Lapsen keskittymisvaikeudet ja ylivilkkaus voivat lisätä vanhemman ja lapsen välisen
vuorovaikutuksen kielteisyyttä ja vanhempien rasittuneisuutta «Flynn MM, Rosen PJ, Reese JS, ym. Examining the in...»177, «Sellers R, Harold GT, Thapar A, ym. Examining the ...»178. Näiden on todettu lievittyvän silloin, kun lapsen oireet vähenevät esimerkiksi hoidon
myötä «Williamson D, Johnston C, Noyes A, ym. Attention-D...»179.
- Oireet saattavat vaikuttaa negatiivisesti myös vanhempien kasvatuskäytäntöihin ja perheen sisäisiin vuorovaikutussuhteisiin «Wells KC, Chi TC, Hinshaw SP, ym. Treatment-relate...»180.
- Lapsen ADHD-oireet voivat lisätä sisarusten välisiä ristiriitoja «Mikami AY, Pfiffner LJ. Sibling relationships amon...»181, «Peasgood T, Bhardwaj A, Biggs K, ym. The impact of...»182.
- Sisarukset saattavat kokea, että he saavat vähemmän huomiota, tulevat kohdelluiksi
epäoikeudenmukaisesti ja joutuvat ottamaan liikaa vastuuta «King K, Alexander D, Seabi J. Siblings' Perception...»183, «Schumann A, Vatne TM, Fjermestad KW. What challeng...»184.
- Lisätietoa Tukiliiton Erityinen sisaruus -sivuilta «https://www.tukiliitto.fi/toiminta/erityinen-sisaruus/»7.
- Sisarukset saattavat kokea, että he saavat vähemmän huomiota, tulevat kohdelluiksi
epäoikeudenmukaisesti ja joutuvat ottamaan liikaa vastuuta «King K, Alexander D, Seabi J. Siblings' Perception...»183, «Schumann A, Vatne TM, Fjermestad KW. What challeng...»184.
- Suositus 14: Koko perheen toimintakykyä ja jaksamista tulee aktiivisesti tukea.
Psykososiaaliset hoidot
- Suositus 15: ADHD:n hoidossa suositellaan käytettäväksi ikäryhmän mukaisia psykososiaalisia menetelmiä.
- Käyttäytymisen ohjaamiseen perustuvat hoitomuodot (käyttäytymishoidot) vähentävät
lasten ja nuorten ADHD:n oireita «Käyttäytymisen ohjaukseen perustuvat hoitomuodot (käyttäytymishoidot) vähentävät lasten ja nuorten ADHD-oireita.»A.
- Käyttäytymishoidoissa aikuiset (vanhemmat, opettaja) ohjaavat lasta tai nuorta siten, että toivottu käyttäytyminen lisääntyy. Interventiot voivat sisältää myös erilaisten taitojen harjoittelua (ks. lisätietoa «ADHD ja käyttäytymishoito»52).
- Käyttäytymistä ohjataan myös muokkaamalla ympäristöä toimintakykyä tukevaksi «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123, «AADPA. Australian Evidence-Based Clinical Practice...»124, ks. myös ADHD-oireisiin vaikuttavat ympäristö- ja motivaatiotekijät «ADHD-oireisiin vaikuttavat ympäristö- ja motivaatiotekijät»21
- Käyttäytymisen ohjaukseen perustuvat menetelmät tukevat myös ADHD-diagnoosin saaneiden lasten tunnesäätelytaitoja «Vacher C, Goujon A, Romo L, ym. Efficacy of psycho...»185, «Breaux R, Baweja R, Eadeh HM, ym. Systematic Revie...»186.
- Sosiaalisten taitojen harjoittelun tarve on arvioitava yksilöllisesti. Cochrane-katsauksen mukaan näyttö sosiaalisten taitojen harjoittelun vaikuttavuudesta ADHD-diagnoosin saaneilla lapsilla ja nuorilla on vähäistä «Storebø OJ, Elmose Andersen M, Skoog M, ym. Social...»187.
Vanhemmuustaito-ohjelmat
- Strukturoituihin vanhemmuustaito-ohjelmiin osallistuminen vähentää lapsen vanhemman
arvioimia ADHD-oireita, lisää positiivisia kasvatuskäytäntöjä ja parantaa kokemusta
vanhemmuudesta sekä lapsen ja vanhemman välisestä suhteesta. Vaikutusten suuruus on
pääasiassa kohtalainen «Strukturoituihin vanhemmuustaito-ohjelmiin osallistuminen vähentää lapsen vanhemman arvioimia ADHD-oireita, lisää positiivisia kasvatuskäytäntöjä ja parantaa kokemusta vanhemmuudesta sekä lapsen ja vanhemman välisestä suhteesta. Vaikutusten suuruus on pääasiassa kohtalainen.»A.
- Vanhempainohjausmenetelmien avulla pyritään parantamaan vanhempien keinoja ohjata lapsensa käyttäytymistä ja tukemaan positiivista perheensisäistä vuorovaikutusta. Vanhempainohjaus toteutetaan yleensä ryhmäohjauksena siihen suunnitellun käsikirjan mukaisesti (ks. lisätietoa «Strukturoidut vanhemmuustaito-ohjelmat ja ADHD»53).
Pikkulasten leikkipohjaiset interventiot
- Strukturoidut leikkipohjaiset interventiot todennäköisesti vähentävät vanhempien arvioimia
3–5-vuotiaiden lasten tarkkaamattomuus- ja ylivilkkausoireita ja vahvistavat itsesäätelytaitoja «Strukturoidut leikkipohjaiset interventiot todennäköisesti vähentävät vanhempien arvioimia 3–5-vuotiaiden lasten tarkkaamattomuus- ja yliaktiivisuusoireita ja vahvistavat itsesäätelytaitoja.»B.
- Leikkiin perustuville interventioille (play-based interventions) yhteistä on tarkkaavuuden ja toiminnanohjauksen perustaitojen harjoittelu vanhemman ohjaamien leikkien ja pelien avulla. Leikeissä vahvistetaan lapsen kehittymässä olevia toiminnanohjauksen perustaitoja, esimerkiksi huomion suuntaamista, vuoron odottamista ja vauhdin säätelyä, ks. lisätietoa «Pikkulasten leikkipohjaiset interventiot ADHD-oireiden hoidossa»54.
Varhaiskasvatuksen ja koulun tukitoimet
- Käyttäytymisen ohjaamiseen ja opettamiseen perustuvat tukitoimet
- Koulussa toteutettavat käyttäytymishoitoihin perustuvat tukitoimet (ks. lisätietoa «Varhaiskasvatuksessa ja koulussa toteutettavat ADHD-oireisten lasten ja nuorten tukitoimet»55) vähentävät opettajien arvioimia alakouluikäisten lasten ADHD:n oireita ja parantavat
toimintakykyä koulussa «Koulussa toteutettavat käyttäytymishoitoihin perustuvat tukitoimet vähentävät opettajien arvioimia alakouluikäisten lasten ADHD:n oireita ja parantavat toimintakykyä koulussa.»A. Varhaiskasvatuksessakin ne saattavat lieventää käytösoireita, mutta suomalaista päivähoito-
tai varhaiskasvatusjärjestelmää vastaavista olosuhteista ei ole tutkimusta.
- Varhaiskasvatuksessa tukitoimien tavoite on tukea lapsen toimintakykyä, sosiaalista osallistumista ja kehitystä.
- Koulun tukitoimien tavoitteena on tukea oppilasta opetukseen osallistumisessa ja oppitavoitteiden saavuttamisessa, ja niitä voidaan toteuttaa osana koulun perustoimintaa «Perusopetuksen opetussuunnitelman perusteiden muut...»188, «https://eperusteet.opintopolku.fi/#/fi/perusopetus/419550/tekstikappale/430064»8.
- Koulun tukitoimet suunnitellaan monialaisessa opiskeluhuollon yhteistyössä «https://eperusteet.opintopolku.fi/#/fi/perusopetus/419550/tekstikappale/432935»9.
- Hyväksi todettujen tukitoimien jatkuminen siirtymävaiheessa (päiväkodista kouluun ja yläluokille ja jatko-opintoihin siirryttäessä) on turvattava huolehtimalla riittävästä tiedonkulusta. Tukitoimien riittävyyttä on arvioitava vuosittain.
- Varhaiskasvatuksen, koulun ja jatko-opintopaikkojen henkilökunta tarvitsee riittävää ohjausta tukitoimien suunnitteluun ja toteuttamiseen.
- Koulussa toteutettavat käyttäytymishoitoihin perustuvat tukitoimet (ks. lisätietoa «Varhaiskasvatuksessa ja koulussa toteutettavat ADHD-oireisten lasten ja nuorten tukitoimet»55) vähentävät opettajien arvioimia alakouluikäisten lasten ADHD:n oireita ja parantavat
toimintakykyä koulussa «Koulussa toteutettavat käyttäytymishoitoihin perustuvat tukitoimet vähentävät opettajien arvioimia alakouluikäisten lasten ADHD:n oireita ja parantavat toimintakykyä koulussa.»A. Varhaiskasvatuksessakin ne saattavat lieventää käytösoireita, mutta suomalaista päivähoito-
tai varhaiskasvatusjärjestelmää vastaavista olosuhteista ei ole tutkimusta.
- Organisointitaitojen harjoittelu
- Organisointitaitojen harjoittelu todennäköisesti parantaa ADHD-diagnoosin saaneiden
lasten ja nuorten taitoja huolehtia koulutehtävistä ja opillista suoriutumista kliinisesti
merkittävästi «Organisointitaitojen harjoittelu todennäköisesti parantaa ADHD-diagnoosin saaneiden lasten ja nuorten taitoja huolehtia koulutehtävistä ja opillista suoriutumista kliinisesti merkittävästi.»B.
- Lapsilla ja nuorilla, joilla on ADHD, on usein vaikeuksia työskentelynsä organisoinnissa. Koulutyössä vaikeudet haittaavat erityisesti läksyistä huolehtimista ja oppitunneille valmistautumista.
- Vaikeuksista aiheutuva haitta usein kasvaa itsenäisen työskentelyn vaatimusten lisääntyessä, kun lapsi siirtyy alakoulun myöhemmille luokille ja edelleen yläkouluun ja toisen asteen opintoihin.
- Systemaattista organisointitaitojen harjoittelua voidaan toteuttaa osana koulun erityisopetusta. Sitä voidaan soveltaa myös koulun ulkopuolisessa kuntoutuksessa, ks. lisätietoa «Organisointitaitojen harjoittelu»56.
- Organisointitaitojen harjoittelu todennäköisesti parantaa ADHD-diagnoosin saaneiden
lasten ja nuorten taitoja huolehtia koulutehtävistä ja opillista suoriutumista kliinisesti
merkittävästi «Organisointitaitojen harjoittelu todennäköisesti parantaa ADHD-diagnoosin saaneiden lasten ja nuorten taitoja huolehtia koulutehtävistä ja opillista suoriutumista kliinisesti merkittävästi.»B.
Psykoterapia
- Lasten ja nuorten ADHD:n hoidossa kognitiivisen tai kognitiivis-behavioraalisen psykoterapian
vaikuttavuutta on tutkittu pääasiassa osana monimuotoista psykososiaalista hoitoa «Young S, Amarasinghe JM. Practitioner review: Non-...»161, «Battagliese G, Caccetta M, Luppino OI, ym. Cogniti...»189, «Fabiano GA, Schatz NK, Aloe AM, Pelham WE, Jr., Sm...»190, «Tourjman V, Louis-Nascan G, Ahmed G, ym. Psychosoc...»191 «Markel C. Child-focused psychosocial interventions...»192, «Riise EN, Wergeland GJH, Njardvik U, ym. Cognitive...»193, ks. lisätietoa «Kognitiivisen psykoterapian ja kognitiivisen käyttäytymisterapian menetelmät lasten ja nuorten ADHD:n hoidossa»57. Näissä tutkimuksissa hoidon on arvioitu olevan vaikuttavaa.
- Olennainen osa lapsen terapiaa on työskentely vanhempien kanssa, ja useimmissa tutkimuksissa lapsen hoitoon on liitetty jokin vanhemmuustaito-ohjelma «Battagliese G, Caccetta M, Luppino OI, ym. Cogniti...»189, «Anastopoulos AD. Facilitating parental understandi...»194, «Ranta K, Kauppi A. Lasten ja nuorten kognitiivinen...»195, ks. lisätietoa «Strukturoidut vanhemmuustaito-ohjelmat ja ADHD»53.
- Vain lapsiin kohdistuneista interventioista ei ole riittävästi tutkimustietoa vaikuttavuuden luotettavaa arviointia varten.
- Kognitiivisen tai kognitiivis-behavioraalisen terapian tarve ja mahdollinen hyöty on arvioitava yksilöllisesti ottaen huomioon samanaikaishäiriöt.
- ADHD-diagnoosin saaneilla aikuisilla kognitiivis-behavioraaliset interventiot vähentävät
kliinisesti merkittävästi ADHD-oireita sekä samanaikaisia masennus- ja ahdistuneisuusoireita «ADHD-diagnoosin saaneilla aikuisilla kognitiivis-behavioraaliset interventiot vähentävät kliinisesti merkittävästi ADHD-oireita sekä samanaikaisia masennus- ja ahdistuneisuusoireita»A.
- Tutkitut muodot ovat enimmäkseen ryhmä- ja yksilömuotoisia kognitiivis-behavioraalisen
psykoterapian (CBT) eri muotoja.
- Muista psykoterapioista kuin laajasti määritellyistä kognitiivis-behavioraalisista terapioista ei ole tutkimuksia tehty.
- Tutkitut CBT-interventiot pitävät sisällään perinteisen kognitiivis-behavioraalisen psykoterapian eri muotojen lisäksi muun muassa dialektiseen käyttäytymisterapiaan terapiaan perustuvia interventioita ja mindfulness-interventioita (ks. lisätietoa «Tutkitut kognitiivis-behavioraaliset interventiot aikuisten ADHD:n hoidossa»58).
- Lähes kaikissa tutkituissa interventioissa keskeisiä elementtejä ovat psykoedukaatio sekä taitojen ja kompensaatiokeinojen harjoittelu.
- Internetpohjaisista CBT-interventioista (Suomessa usein nettiterapia-nimikkeellä) on muutamia tutkimuksia, joissa hyötyä on todettu «Pettersson R, Söderström S, Edlund-Söderström K, y...»196, «Nasri B, Cassel M, Enhärje J, ym. Internet deliver...»197
- Mielenterveystalo-sivuston aikuisille suunnattu nettiterapia «https://www.mielenterveystalo.fi/fi/nettiterapiat»10 perustuu CBT-menetelmiin, mutta sen vaikuttavuudesta ei ole julkaistu toistaiseksi tutkimustietoa.
- Tutkitut muodot ovat enimmäkseen ryhmä- ja yksilömuotoisia kognitiivis-behavioraalisen
psykoterapian (CBT) eri muotoja.
- Mindfulness-pohjaiset interventiot saattavat vähentää kohtalaisesti lasten ja nuorten ADHD-oireita «Mindfulness-pohjaiset interventiot saattavat vähentää kohtalaisesti lasten ja nuorten ADHD-oireita.»C.
- Muista terapiamuodoista ei ole riittävästi tutkimustietoa, jotta niiden vaikuttavuutta lasten, nuorten tai aikuisten ADHD-oireisiin voitaisiin arvioida.
Neuropsykologinen kuntoutus
- Neuropsykologinen kuntoutus voi olla hyödyllistä tarkkaavuuden, toiminnanohjauksen,
muistin ja liitännäisoireina ilmenevien oppimisvaikeuksien takia, jos henkilöllä on
merkittävää toimintakykyhaittaa.
- Neuropsykologinen kuntoutus (ks. lisätietoa «Neuropsykologinen kuntoutus ja ADHD»36) kohdistuu ADHD-oireisiin sekä käyttäytymisessä ja kognitiivisissa tai muissa psyykkisissä toiminnoissa ilmeneviin vaikeuksiin.
- Neuropsykologinen kuntoutus suunnitellaan yksilöllisesti, ja se sisältää muun muassa psykoedukaatiota, kognitiivis-behavioraalisen psykoterapian ja käyttäytymishoitojen menetelmiä sekä strategioiden (erityisesti toiminnanohjauksen) harjoittelua.
- ADHD-oireisten lasten ja nuorten neuropsykologisen kuntoutuksen olennainen osa on opettajille ja huoltajille annettava ohjaus.
- Suomessa käytössä olevan kokonaisvaltaisen, yksilöllisen neuropsykologisen kuntoutuksen vaikuttavuudesta ADHD:ssä ei ole tutkimuksia. Lähin tutkimustieto aikuisten osalta on kognitiivis-behavioraalisista, ADHD-oireisille mukautetuista hoitomuodoista «ADHD-diagnoosin saaneilla aikuisilla kognitiivis-behavioraaliset interventiot vähentävät kliinisesti merkittävästi ADHD-oireita sekä samanaikaisia masennus- ja ahdistuneisuusoireita»A, lasten ja nuorten osalta myös käyttäytymishoidoista «Käyttäytymisen ohjaukseen perustuvat hoitomuodot (käyttäytymishoidot) vähentävät lasten ja nuorten ADHD-oireita.»A ja organisointitaitojen harjoittelusta «Organisointitaitojen harjoittelu todennäköisesti parantaa ADHD-diagnoosin saaneiden lasten ja nuorten taitoja huolehtia koulutehtävistä ja opillista suoriutumista kliinisesti merkittävästi.»B.
- Neuropsykologista kuntoutusta voidaan toteuttaa myös ryhmämuotoisena.
Toimintaterapia
- Toimintaterapiasta ADHD:n hoidossa ei ole riittävästi tutkimuksia vaikuttavuuden arvioimiseksi.
Toimintaterapia voi kuitenkin olla tarpeen osana yksilöllistä kuntoutusta.
- Toimintaterapia on toiminnan, neuvonnan ja ohjauksen avulla annettavaa lääkinnällistä kuntoutusta, jolla tuetaan toimintakykyä ja omatoimisuutta sekä lapsilla myös kokonaiskehitystä sekä motorisia ja hahmottamisvalmiuksia.
- Toimintaterapia voidaan toteuttaa yksilö- tai ryhmäterapiana, ja lasten toimintaterapiaan kuuluu myös aikuisten ohjausta (esim. vanhemmat, koulu).
- Toimintaterapialla voidaan edistää erilaisia taitoja ja valmiuksia sekä ympäristössä toimimista. Sillä voi olla myönteisiä vaikutuksia ADHD-oireisen lapsen toiminnalliseen suoriutumiseen tai sosiaalisiin taitoihin (ks. lisätietoa «Toimintaterapia ADHD:n hoidossa»59), «Novak I, Honan I. Effectiveness of paediatric occu...»198. Aikuisilla toimintaterapia voi tukea oirehallintaa ja toimintakykyä «Adamou M, Asherson P, Arif M, ym. Recommendations ...»199.
- Osalla ADHD-oireisista lapsista voi syntyä tarve toimintaterapiakuntoutukseen samanaikaisen kehityksellisen koordinaatiohäiriön (ks. Käypä hoito -suositus Lasten ja nuorten kehityksellinen koordinaatiohäiriö (DCD) «Lasten ja nuorten kehityksellinen koordinaatiohäiriö (DCD)»8, «Lasten ja nuorten kehityksellinen koordinaatiohäir...»139) tai aistitiedon käsittelyn ja säätelyn vaikeuksien (ks. lisätietoa «Aistitiedon käsittelyn vaikeudet ja ADHD»60) vuoksi.
Neuropsykiatrinen valmennus
- Neuropsykiatrisesta valmennuksesta ADHD-oireiden hoidossa ei ole riittävästi tutkimustietoa
vaikuttavuuden arvioimiseksi.
- Vuonna 2022 julkaistussa Australian ADHD-hoitosuosituksessa suositellaan neuropsykiatrisen valmennuksen tarjoamista nuorille ja aikuisille osana ADHD:n kokonaishoitoa, vaikka suora tutkimusnäyttö on vähäistä. Suositusta on perusteltu sillä, että valmennus sisältää samoja ympäristön muokkaamisen, kognitiivis-behavioraalisen terapian ja käyttäytymisen ohjaamisen menetelmiä, joiden vaikuttavuus on osoitettu muissa tutkimuksissa «AADPA. Australian Evidence-Based Clinical Practice...»124. Australiassa ja Suomessa käytetyt menetelmät saattavat poiketa toisistaan.
- Neuropsykiatrinen valmennus on arkiympäristössä toteutuvaa asiakkaan ohjausta, jonka
tavoitteena on vahvistaa uusien toiminta- ja ratkaisumallien löytämistä, tukea oirehallintaa
tukevien menetelmien käyttöön ottamista sekä toiminnanohjauksen ja arjen hallinnan
taitojen harjoittelua «AADPA. Australian Evidence-Based Clinical Practice...»124, «Nyfors H. Selvitys neuropsykiatrisen valmennuksen ...»200. Ks. lisätietoa «ADHD ja neuropsykiatrinen valmennus»61.
- Valmennusta voi toteuttaa esimerkiksi sosiaali- ja terveysalan tai opetus- ja kasvatusalan ammattilainen, jolla on neuropsykiatrisen valmentajan täydennyskoulutus. Koulutusten sisällöissä ja valmentajien ammattitaustassa on kuitenkin vaihtelua, eikä valmennus ole sisällöltään vakioitua.
- Valmennus voi toteutua muutamana ohjauskäyntinä esimerkiksi osana terveydenhuollon
yksikön antamaa diagnoosin jälkeistä psykoedukatiivista ohjausta tai tavoitteellisena
pidempänä valmentavana jaksona «Nyfors H. Selvitys neuropsykiatrisen valmennuksen ...»200.
- Pidemmän valmennusjakson tarve on harkittava yksilöllisesti, ja työskentelylle tulee asettaa selkeät tavoitteet.
- Lasten ja nuorten neuropsykiatrinen valmennus tapahtuu yhdessä vanhempien kanssa tai vanhempia valmentamalla.
- Kliinisen kokemuksen perusteella valmennus vaikuttaa soveltuvan kuntoutuksen menetelmäksi esimerkiksi tilanteissa, joissa tarvitaan käytännönläheistä ohjaamista oirehallinnan menetelmien käyttöönotossa.
Lääkehoito
- Suositus 16: Lääkehoito voi olla tarpeen osana hoidon kokonaisuutta. Sen tarvetta
arvioidaan, kun diagnoosi varmistunut, ja etenkin jos muut tuki- ja hoitomuodot osoittautuvat
riittämättömiksi tai oireet ovat niin vaikeita, että muiden hoitomuotojen toteuttaminen
ei onnistu
«Faraone SV, Banaschewski T, Coghill D, ym. The Wor...»11, «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123, «AADPA. Australian Evidence-Based Clinical Practice...»124, «Wolraich ML, Hagan JF Jr, Allan C, ym. Clinical Pr...»151, «Mechler K, Banaschewski T, Hohmann S, ym. Evidence...»152, «Sibley MH, Flores S, Murphy M, ym. Research Review...»155, «Catalá-López F, Hutton B, Núñez-Beltrán A, ym. The...»201, «Van Vyve L, Dierckx B, Lim CG, ym. Pharmacotherapy...»203, «Cortese S, Adamo N, Del Giovane C, ym. Comparative...»204, «O'Connor L, Carbone S, Gobbo A, ym. Pediatric atte...»205.
- Tarpeellisia tukitoimia ja psykososiaalisia hoitomuotoja jatketaan lääkehoidon aikana.
- Ks. video ADHD:n lääkehoito voi olla tarpeen osana hoidon kokonaisuutta «ADHD:n lääkehoito voi olla tarpeen osana hoidon kokonaisuutta (video)»5.
- Vaikka suurin osa suomalaisista käyttää ADHD-lääkkeensä ohjeen mukaan, on hoitoa suunniteltaessa ja hoitovastetta arvioitaessa huomioitava, että ADHD-lääkkeiden väärinkäyttö on mahdollista. Väärinkäytön riskiä voi kuitenkin vähentää käytännön toimilla, esimerkiksi valitsemalla pitkävaikutteisia valmisteita sekä reseptinmääräämiskäytännöin. Ks. lisätietoa «ADHD-lääkkeiden väärinkäytön riski»62.
- ADHD:n lääkehoidot ovat yleistyneet, ja lääkehoitojen yleisyydessä on huomattavia alueellisia eroja, ks. lisätietoa ADHD:n ja lääkehoidon yleisyyttä koskevat tutkimukset Suomessa «ADHD:n ja lääkehoidon yleisyyttä koskevat tutkimukset Suomessa»8.
- Tarpeellisia tukitoimia ja psykososiaalisia hoitomuotoja jatketaan lääkehoidon aikana.
- Valviran ohjeen mukaan lääkehoidon voi aloittaa (ks. Valvira «https://valvira.fi/sosiaali-ja-terveydenhuolto/adhd-ja-laakkeiden-maaraaminen»11)
- lapsilla ja nuorilla lasten- tai nuorisopsykiatri, lastenlääkäri tai -neurologi tai
muu lasten tai nuorten psyykkiseen ja fyysiseen kehitykseen ja ADHD:n hoitoon perehtynyt
lääkäri tai vastaavien alojen erikoistuva lääkäri erikoistumispaikassaan
- Alle 6-vuotiaiden lasten lääkehoito (ks. lisätietoa «Alle kouluikäisten lasten ADHD:n lääkehoito»63) vaatii erityistä huolellisuutta (ks. hoidon porrastus «A4»6).
- aikuisilla psykiatrian tai neurologian alojen erikoislääkäri. Lääkehoitoa voi jatkaa myös muu ADHD:n hoitoon perehtynyt lääkäri tai vastaavien alojen erikoistuva lääkäri erikoistumispaikassaan.
- Tarkista ajankohtaiset viranomaisten antamat määräysohjeet, ks. Fimea «https://fimea.fi/valvonta/lait_ja_ohjeet/maaraykset»12.
- lapsilla ja nuorilla lasten- tai nuorisopsykiatri, lastenlääkäri tai -neurologi tai
muu lasten tai nuorten psyykkiseen ja fyysiseen kehitykseen ja ADHD:n hoitoon perehtynyt
lääkäri tai vastaavien alojen erikoistuva lääkäri erikoistumispaikassaan
- Suositus 17: Mikäli lääkehoito aloitetaan, sen seurannan täytyy olla systemaattista ja erityisesti alussa riittävän tiivistä vasteen, tarpeen ja haittavaikutusten arvioimiseksi.
- Lääkkeen valinnassa (ks. lisätietoa ADHD:n hoidossa käytettävät lääkkeet «ADHD:n hoidossa käytettävät lääkkeet»64 ja ADHD-lääkevalmisteen valinta «ADHD-lääkevalmisteen valinta»65, «Metyylifenidaattivalmisteiden vaikutusprofiilit»3) tulee ottaa huomioon oireiden esiintyminen eri tilanteissa ja eri vuorokaudenaikoina
ja mahdolliset muut samanaikaiset ongelmat.
- Lääkevalmisteen valintaan vaikuttaa se, kuinka nopeaa ja pitkävaikutteista vastetta toivotaan.
- Valmisteen valintaan voivat vaikuttaa erot suurimman tehon ajoittumisessa, lääkkeen ottamiseen (erityisesti lapsilla nielaisemiseen) liittyvät vaikeudet sekä lääkkeiden määräämiseen liittyvät ohjeet «https://fimea.fi/laakehaut_ja_luettelot/laakehaku»13, «Puustjärvi A, Putkonen H, Sumia M ym. ADHD:n lääke...»202, «Van Vyve L, Dierckx B, Lim CG, ym. Pharmacotherapy...»203, «Cortese S, Adamo N, Del Giovane C, ym. Comparative...»204 «O'Connor L, Carbone S, Gobbo A, ym. Pediatric atte...»205.
- Saatavilla olevista lääkkeistä valitaan oirehallinnan kannalta tilanteeseen parhaiten
sopiva valmiste.
- Lasten ja nuorten ensisijainen aloituslääke on useimmiten keskipitkä- tai pitkävaikutteinen metyylifenidaatti.
- Aikuisten ensisijainen lääke voi olla metyylifenidaatti, atomoksetiini tai lisdeksamfetamiini. Lääke valitaan yksilöllisen harkinnan perusteella.
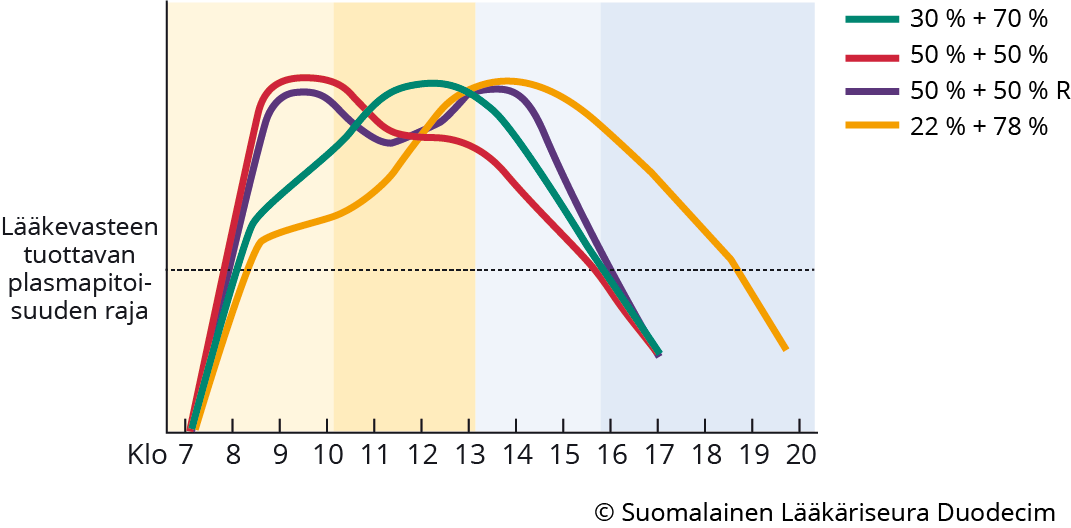
Metyylifenidaattivalmisteiden välillä on eroa siinä, kuinka paljon niissä on nopeasti ja hitaasti vapautuvaa lääkemuotoa. Lääkeaineen vapautuminen vaikuttaa lääkeainepitoisuuteen elimistössä ja siten myös siihen, mihin aikaan päivästä lääkkeen teho on suurin. Siihen, mitä alkuperäisvalmistetta rinnakkaisvalmiste vastaa, kannattaa kiinnittää erityistä huomiota. Kuvio esittää eri lääkevalmisteiden erot kaavamaisesti. Pystyakselin arvot ovat suhteellisia, eivät seerumipitoisuuksia.
- 30 % + 70 % -valmiste: vahvuudet 10 mg, 20 mg, 30 mg
- 50 % + 50 % -valmiste: vahvuudet 5 mg, 10 mg, 20 mg, 30 mg, 40 mg, 50 mg, 60 mg
- 50 % + 50 % -valmiste: (viiveellä vapautuva 50 %, bimodaalinen vapautuminen): vahvuudet 20 mg, 30 mg, 40 mg ja 60 mg
- 22 % + 78 % -valmiste: vahvuudet 18, 27, 36 ja 54 mg
Lähteet: Fimea lääketietokanta «https://fimea.fi/laakehaut_ja_luettelot/laakehaku»13
Banaschewski T, Coghill D, Santosh P, ym. Long-acting medications for the hyperkinetic disorders. A systematic review and European treatment guideline. Eur Child Adolesc Psychiatry 2006;15(8):476-95 «PMID: 16680409»PubMed
- Lääkehoitoa aloitettaessa sovitaan, mitä oireita ja toimintakyvyn muutoksia seurataan.
- Tehoa ja haittavaikutuksia arvioidaan haastatteluin ja kyselylomakkein (esim. ADHD-oirelomakkeen täyttäminen ennen lääkehoitoa ja sen aikana oireissa tapahtuvan muutoksen arvioimiseksi «hoi50061d.pdf»1, «hoi50061c.pdf»6).
- Laboratoriokokeita ei tarvita, ellei potilaan muu terveydentila sitä edellytä (esim. epäily maksan, munuaisten tai kilpirauhasen toimintahäiriöstä).
- Sekä lapsilla että aikuisilla on arvioitava esitietojen ja nykytilan tutkimuksella, esiintyykö sellaisia sydän- ja verenkiertoelinten sairauksia, jotka voivat vaikeutua ADHD-lääkehoidon mahdollisista haittavaikutuksista.
- Lääkitys aloitetaan pienellä annoksella, minkä jälkeen annosta suurennetaan tarvittaessa
yksilöllisen vasteen mukaisesti 1–2 viikon välein vähitellen hoitovastetta ja haittavaikutuksia
seuraten «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123, «AADPA. Australian Evidence-Based Clinical Practice...»124, «Van Vyve L, Dierckx B, Lim CG, ym. Pharmacotherapy...»203, «Cortese S, Adamo N, Del Giovane C, ym. Comparative...»204, «O'Connor L, Carbone S, Gobbo A, ym. Pediatric atte...»205 . Tavoitteena on löytää pienin mahdollinen vuorokausiannos, jolla saavutetaan hyvä
teho ilman merkittäviä haittavaikutuksia. Myöhemmin mahdollisen lääketauon jälkeen
voidaan lääkehoitoa jatkaa suoraan tehokkaaksi todetulla hoitoannoksella.
- Ellei yksilöllisestä annoksen säädöstä (annoksen riittävä suurentaminen, vaihto tai yhdistäminen eri vaikutusprofiilin tai -ajan valmisteeseen) huolimatta saada riittävää vastetta, kokeillaan toista lääkeainetta.
- Jos millään yksittäisellä lääkeaineella ei saavuteta riittävää vastetta, voidaan harkitusti kokeilla lääkkeiden käyttöohjeista poikkeavaa annostelua tai yhdistää erilaisia lääkevalmisteita. Tämä vaatii erityistä osaamista, tarkkaa haittavaikutusten seurantaa ja toteutetaan yleensä erikoissairaanhoidossa «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123, «Van Vyve L, Dierckx B, Lim CG, ym. Pharmacotherapy...»203, «Hammerness P, Georgiopoulos A, Doyle RL, ym. An op...»207, ks. lisätietoa ADHD-lääkevalmisteen valinta «ADHD-lääkevalmisteen valinta»65.
- Suositus 18: Hyvän hoitovasteen saavuttamisen jälkeen lääkehoitoa arvioidaan säännöllisesti
yksilöllisen tarpeen mukaan, alussa tiiviisti ja jatkossakin kuitenkin vähintään kerran
vuodessa.
- Arvion yhteydessä tarkistetaan kokonaistilanne, lääkeannoksen teho ja riittävyys sekä lääkityksen jatkamisen tarve «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123, «Van Vyve L, Dierckx B, Lim CG, ym. Pharmacotherapy...»203, «O'Connor L, Carbone S, Gobbo A, ym. Pediatric atte...»205, «European Medicines Agency. Questions and answers o...»208.
- Lääkehoidon aikana seurataan sykettä ja verenpainetta sekä lapsilla ja nuorilla painon ja pituuden kehitystä kasvukäyrien avulla lääkehoidon alkuvaiheessa ja muuttuessa 3–6 kuukauden välein (ks. lisätietoa «Tavallisten haittavaikutusten ja yksilöllisten riskien huomiointi ADHD:n lääkehoidossa»66).
- Osa ADHD-diagnoosin saaneista lapsista ja nuorista tarvitsee lääkehoitoa aikuisiässäkin,
osalla lääkehoito voidaan lopettaa oireiden lievittymisen ja uusien taitojen oppimisen
myötä «Coghill D, Banaschewski T, Cortese S, ym. The mana...»118, «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «Wolraich ML, Hagan JF Jr, Allan C, ym. Clinical Pr...»151.
- Lääkehoito voidaan aloittaa tarvittaessa myöhemmin uudelleen tai myös ensimmäistä kertaa vasta aikuisiässä.
- Lääkehoidon tehon ja tarpeen arvioimiseksi voidaan stimulanttilääkehoidossa pitää
lääketauko.
- Lääketauko kannattaa ajoittaa siten, että toimintakyvyn ja oireiden arviointi on luotettavaa. Tauon ajoittamisessa on otettava huomioon muut mahdollisesti toimintakykyä muuttavat samanaikaiset seikat tai muutokset. Koulujen loma-aikana pidetty lääketauko ei välttämättä anna luotettavaa käsitystä lapsen tai nuoren ADHD-oireiden muutoksesta tai toimintakyvystä.
- Jos lääketauon aikana oireet eivät aiheuta merkittävää haittaa, voidaan lääkehoito yleensä lopettaa. Muita hoito- ja tukimuotoja kannattaa kuitenkin jatkaa.
- Jos lääketauon aikana ADHD-oireista on edelleen selvää haittaa toimintakyvylle, jatketaan lääkehoitoa aiemmalla tai tarkistetulla annoksella.
- Lääkehoito tulee lopettaa, jos ilmenee selviä haittavaikutuksia, joita ei voida lääkemuutoksella hallita, tai herää epäily lääkkeen väärinkäytöstä.
- Tiedot yleisimpien ADHD:n hoidossa käytettävien lääkkeiden annoksista, vaikutusajasta ja muista huomioon otettavista asioista esitetään lääketaulukossa «ADHD:n hoidossa käytettävät lääkkeet»64.
- Lääkehoitoa on mahdollista käyttää raskauden ja imetyksen aikana silloin, kun se ADHD-oireiden
vaikeuden vuoksi on välttämätöntä ja kun hoidosta odotettavissa oleva hyöty on suurempi
kuin sikiölle ja lapselle mahdollisesti aiheutuva riski, ks. lisätietoa «ADHD:n lääkehoito raskauden ja imetyksen aikana»67. Lääkityksessä pyritään löytämään mahdollisimman pieni vaikuttava hoitoannos «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123, «Ornoy A, Koren G. The Effects of Drugs used for th...»209, «Scoten O, Tabi K, Paquette V, ym. Attention-defici...»210, «National Library of Medicine. Drugs and Lactation ...»211.
- ADHD-lääkitys raskauden aikana:
- Suomessa aikuisten ADHD:n hoidossa käytetyistä lääkkeistä metyylifenidaatti, atomoksetiini ja lisdeksamfetamiini ovat mahdollisia «di Giacomo E, Confalonieri V, Tofani F, ym. Methyl...»212, «Bang Madsen K, Robakis TK, Liu X, ym. In utero exp...»213. Guanfasiinista ei ole tutkimustietoa.
- ADHD-lääkitys imetyksen aikana:
- Metyylifenidaatti on lääkkeistä tutkituin. Se kulkeutuu hoitoon käytettyinä annoksina rintamaitoon vain pieninä pitoisuuksina ja vaikuttaa tapausselostusten perusteella turvalliselta «National Library of Medicine. Drugs and Lactation ...»211.
- Metyylifenidaatti saattaa vähentää prolaktiinin määrää, joten imetyksen onnistumista ja myös imeväisen mahdollisia oireita tulee seurata huolellisesti.
- Amfetamiinijohdannaiset kulkeutuvat rintamaitoon «National Library of Medicine. Drugs and Lactation ...»211. Suomessa aikuisille määrätyistä lääkkeistä lisdeksamefetamiinin tai atomoksetiinin käytöstä imettäessä ei ole tutkimustietoa.
- ADHD-lääkitys raskauden aikana:
Stimulantit
- Metyylifenidaatti (MPH) vähentää kliinisesti merkittävästi lasten ja nuorten ADHD:n
tarkkaamattomuus-, impulsiivisuus- ja yliaktiivisuusoireita ainakin lyhytaikaisessa (alle puolen vuoden) hoidossa «Metyylifenidaatti (MPH) vähentää kliinisesti merkittävästi lasten ja nuorten ADHD:n tarkkaamattomuus-, impulsiivisuus- ja yliaktiivisuusoireita ainakin lyhytaikaisessa käytössä.»A, ja se vähentää myös aikuisten ADHD-oireita enemmän kuin lumelääke «Metyylifenidaatti (MPH) vähentää aikuisten ADHD:n oireita enemmän kuin lumelääke.»A.
- Metyylifenidaatti suurentaa dopamiini- ja noradrenaliinipitoisuutta synapsiraossa estämällä presynaptisia dopamiinin ja noradrenaliinin kuljettajaproteiineja (DAT ja NET) «Van Vyve L, Dierckx B, Lim CG, ym. Pharmacotherapy...»203, «Korkeila J, Leppämäki S. ADHD. Kirjassa: Psykiatri...»214, «Stahl S. Stahl´s Essential Psychopharmacology. Neu...»215.
- Deks- ja lisdeksamfetamiini vähentävät lasten ja nuorten ADHD:n oireita lumelääkkeeseen verrattuna «Deksamfetamiini ja lisdeksamfetamiini vähentävät lasten ja nuorten ADHD:n oireita lumelääkkeeseen verrattuna.»A. Lisdeksamfetamiini vähentää aikuisten ADHD:n oireita alle puolen vuoden kestoisessa
hoidossa «Lisdeksamfetamiini vähentää aikuisten ADHD:n oireita enemmän kuin lumelääke alle puolen vuoden kestoisessa hoidossa.»A ja saattaa vähentää ADHD:n oireita vähintään puolen vuoden kestoisessa hoidossa
«Lisdeksamfetamiini saattaa vähentää aikuisten ADHD:n oireita vähintään puolen vuoden kestoisessa hoidossa enemmän kuin lumelääke.»C lumelääkkeeseen verrattuna.
- Amfetamiinien vaikutusmekanismina arvellaan olevan kompetitiivinen dopamiini- ja noradrenaliinitransporttereiden esto sekä dopamiinin vapautuminen presynaptisesta hermopäätteestä synapsiin «Van Vyve L, Dierckx B, Lim CG, ym. Pharmacotherapy...»203, «Korkeila J, Leppämäki S. ADHD. Kirjassa: Psykiatri...»214, «Stahl S. Stahl´s Essential Psychopharmacology. Neu...»215.
- Stimulanttilääkkeistä on käytettävissä lyhyt- (2–6 tuntia), keskipitkä- (6–8 tuntia)
ja pitkävaikutteisia valmisteita (8–14 tuntia), ks. lisätietoa ADHD-lääkevalmisteen
valinta «ADHD-lääkevalmisteen valinta»65.
- Lääkkeen vaikutus voi olla havaittavissa nopeasti (jo ensimmäisenä hoitopäivänä) pienelläkin annoksella, mutta hoidollisesti optimaalinen annos on etsittävä yksilöllisesti annosta riittävästi suurentamalla.
- Lääkitystä on mahdollista käyttää jatkuvasti (päivittäin) tai taukoja (esim. viikonloppuisin tai lomilla) pitäen.
Atomoksetiini
- Atomoksetiini vähentää lasten ja nuorten «Atomoxetine compared to placebo improves the core symptoms of ADHD (inattention, impulsivity and hyperactivity) in children and adolescents at least in the short-term (less than half a year) treatment.»A ja myös aikuisten «Atomoksetiini verrattuna lumeeseen vähentää aikuisten ADHD-oireita lyhytaikaisessa, alle 6 kuukauden hoidossa.»A ADHD-oireita ainakin lyhytkestoisessa (alle puolen vuoden) hoidossa
- Atomoksetiini on selektiivinen noradrenaliinin takaisinoton estäjä «Van Vyve L, Dierckx B, Lim CG, ym. Pharmacotherapy...»203, «Korkeila J, Leppämäki S. ADHD. Kirjassa: Psykiatri...»214, «Stahl S. Stahl´s Essential Psychopharmacology. Neu...»215. Lääkkeen metaboloitumisessa on geneettisiä eroja (CYP2D6), jotka voivat vaikuttaa lääkkeen plasmapitoisuuteen.
- Atomoksetiinia käytetään jatkuvana, päivittäin otettavana lääkityksenä, ja sen teho on ympärivuorokautinen.
- Vaikutus alkaa yleensä 2–6 viikon kuluessa. Vaikutus voi voimistua 8.–12. hoitoviikkoon saakka.
Guanfasiini
- Guanfasiini vähentää lyhytkestoisessa hoidossa lasten ja nuorten ADHD:n oireita, mutta tutkimuksia pitkäaikaisesta käytöstä ei ole «Guanfasiini vähentää lyhytkestoisessa hoidossa lasten ja nuorten ADHD:n oireita, mutta tutkimuksia pitkäaikaisesta käytöstä ei ole.»A. Guanfasiini saattaa lievittää aikuisten ADHD:n oireita lumelääkettä enemmän lyhytkestoisessa, korkeintaan kolme kuukautta kestävässä hoidossa
«Guanfasiini saattaa lievittää aikuisten ADHD:n oireita lumelääkettä enemmän lyhytkestoisessa, korkeintaan kolme kuukautta kestävässä hoidossa.»C.
- Guanfasiini on adrenerginen alfa2-agonisti «Stahl S. Stahl´s Essential Psychopharmacology. Neu...»215.
- Guanfasiinia käytetään jatkuvana, päivittäin otettavana lääkityksenä, ja sen teho on ympärivuorokautinen.
- Vaikutus alkaa yleensä 1–3 viikon kuluessa.
- Guanfasiinin äkilliseen lopettamiseen liittyy verenpaineen nousun ja harvinaisen enkefalopatian riski, ja se on lopetettava asteittain vähentäen.
- Guanfasiinin virallisena käyttöaiheena on lasten ja nuorten ADHD:n hoito, joten lääkkeen määrääminen aikuisille on käyttöaiheen vastaista ja edellyttää erityistä perehtyneisyyttä ADHD:n lääkehoitoon.
ADHD-lääkkeiden haittavaikutukset
- Metyylifenidaatin ja amfetamiinijohdosten haittavaikutukset ovat lasten, nuorten ja aikuisten ADHD:n lyhytkestoisessa hoidossa
tavallisia mutta yleensä lieviä «Metyylifenidaatin ja amfetamiinijohdosten haittavaikutukset ovat lasten ja nuorten ADHD:n lyhytkestoisessa hoidossa tavallisia mutta yleensä lieviä.»A.
- Tavallisimpia haittavaikutuksia ovat ruokahaluttomuus, verenpaineen nousu, syketaajuuden suureneminen, univaikeudet, päänsärky ja vatsakivut.
- Vakavat haittavaikutukset ovat harvinaisia, mutta niille altistavat yksilölliset riskit on otettava huomioon (ks. lisätietoa «Tavallisten haittavaikutusten ja yksilöllisten riskien huomiointi ADHD:n lääkehoidossa»66).
- Atomoksetiinin haittavaikutukset ovat tavallisia mutta yleensä lieviä ainakin lyhytkestoisessa
hoidossa lapsilla ja nuorilla «Adverse reactions of atomoxetine in short-term treatment in children and adolescents are common but usually mild.»A.
- Tavallisimpia ilmoitettuja haittavaikutuksia ovat heikentynyt ruokahalu, ohimenevät ruoansulatuskanavan oireet, verenpaineen nousu, syketaajuuden suureneminen sekä ohimenevä väsymys (ks. lisätietoa «Tavallisten haittavaikutusten ja yksilöllisten riskien huomiointi ADHD:n lääkehoidossa»66).
- ADHD:n hoito atomoksetiinilla, guanfasiinilla, amfetamiineilla tai metyylifenidaatilla ei ilmeisesti lisää vakavien sydänperäisten haittavaikutusten riskiä «ADHD:n hoito atomoksetiinilla, guanfasiinilla, amfetamiinilla tai metyylifenidaatilla ei ilmeisesti lisää vakavien sydänperäisten haittavaikutusten riskiä.»B.
- Guanfasiinin haittavaikutuksina esiintyy uneliaisuutta, väsymystä sekä vireystilan, verenpaineen ja syketaajuuden laskua. Se voi myös aiheuttaa ruokahalun muutoksia, usein ruokahalun lisääntymistä ja siihen liittyvää painon nousua (ks. lisätietoa «Tavallisten haittavaikutusten ja yksilöllisten riskien huomiointi ADHD:n lääkehoidossa»66).
- Harvinaisempia ja pitkäaikaiseen käyttöön liittyviä haittavaikutuksia on kuvattu tarkemmin lisätietoaineistossa Tavallisten haittavaikutusten ja yksilöllisten riskien huomiointi ADHD:n lääkehoidossa «Tavallisten haittavaikutusten ja yksilöllisten riskien huomiointi ADHD:n lääkehoidossa»66.
Muut lääkkeet
- Seuraavilla lääkkeillä ei Suomessa ole käyttöaihetta ADHD:hen, eikä niitä suositella
käytettäväksi ilman erikoissairaanhoidossa tehtyä arviota.
- Klonidiini ilmeisesti vähentää lasten ja nuorten ADHD:n keskeisiä oireita lyhytkestoisessa hoidossa
«Klonidiini ilmeisesti vähentää lasten ja nuorten ADHD:n oireita lyhytaikaisessa hoidossa.»B, mutta tutkimustuloksia pitkäkestoisesta hoidosta ei ole.
- Klonidiini on adrenerginen alfa2-agonisti, jonka virallisena käyttöaiheena Suomessa on kohonnut verenpaine.
- Klonidiinin vaikutuksesta aikuisten ADHD:n oireisiin ei ole riittävästi tutkimustietoa tehon arvioimiseksi. Kliinisen kokemuksen perusteella klonidiini saattaa lievittää joidenkin aikuisten ADHD:n oireita, erityisesti jos samanaikaisesti esiintyy tic-oireita tai Touretten oireyhtymä.
- Klonidiinilla on suhteellisen runsaasti haittavaikutuksia (väsyneisyyttä, uneliaisuutta ja suun kuivumista), ja sinusbradykardiaa on esiintynyt noin neljänneksellä potilaista. Myös QT-ajan pidentymistä on kuvattu.
- Modafiniili ei vähentäne aikuisten ADHD:n oireita enempää kuin lumelääke lyhytaikaisen hoidon
aikana «Modafiniili ei vähentäne aikuisten ADHD:n oireita enempää kuin lumelääke lyhytaikaisen, korkeintaan 9 viikon kestoisen hoidon aikana.»C. Pitkäaikaiskäytöstä ei ole tutkimustietoa.
- Modafiniilia ei sen turvallisuuteen liittyvien seikkojen vuoksi pidä käyttää alle 18-vuotiaiden ADHD:n hoitoon.
- Euroopan lääkevirasto (European Medicines Agency, EMA) «https://www.ema.europa.eu/en/medicines/human/referrals/modafinil»14 julkaisi heinäkuussa 2010 suosituksen, jonka mukaan modafiniilia tulisi käyttää ainoastaan narkolepsian hoitoon.
- Venlafaksiini ei näyttäisi vähentävän aikuisten ADHD-oireita lyhytaikaisessa hoidossa lumelääkettä enemmän, mutta luotettava tutkimusnäyttö asiasta puuttuu «Venlafaksiini ei näyttäisi vähentävän aikuisten ADHD-oireita lyhytaikaisessa hoidossa enempää kuin lumelääke, mutta luotettava tutkimusnäyttö puuttuu.»D.
- Bupropioni saattaa vähentää aikuisten ADHD:n oireita enemmän kuin lumelääke lyhytkestoisessa hoidossa «Bupropioni saattaa vähentää aikuisten ADHD:n oireita enemmän kuin lumelääke, ainakin lyhytaikaisessa hoidossa. Vaikutuksen suuruus on vähäinen tai kohtalainen ja saattaa olla kliinisesti merkittävä.»C. Vaikutuksen suuruus on vähäinen tai kohtalainen ja saattaa olla kliinisesti merkittävä. Lasten ja nuorten hoidossa siitä saattaa olla vähäistä hyötyä verrattuna lumelääkkeeseen «Bupropionista saattaa olla vähäistä hyötyä lasten ja nuorten ADHD-oireiden hoidossa verrattuna lumelääkkeeseen, mutta luotettava näyttö puuttuu.»D, mutta luotettava näyttö puuttuu. Bupropioni ei ole FDA:n hyväksymä lasten ja nuorten hoidossa mihinkään käyttöaiheeseen.
- Klonidiini ilmeisesti vähentää lasten ja nuorten ADHD:n keskeisiä oireita lyhytkestoisessa hoidossa
«Klonidiini ilmeisesti vähentää lasten ja nuorten ADHD:n oireita lyhytaikaisessa hoidossa.»B, mutta tutkimustuloksia pitkäkestoisesta hoidosta ei ole.
Muut hoidot
- Suositus 19: Työryhmä suosittaa liikuntaa ADHD-oireiden lievittämiseen. Liikunta ilmeisesti vähentää lasten ja nuorten ADHD:n keskeisiä oireita «Liikunta ilmeisesti vähentää lasten ja nuorten ADHD:n keskeisiä oireita.»B. Aikuisten osalta tutkimuksia ei ole tehty tarpeeksi vaikuttavuuden arvioimiseksi.
- Transkraniaalinen tasavirtastimulaatio saattaa lievittää ADHD-oireita lumestimulaatiota enemmän välittömästi hoidon jälkeen, mutta vaikutus on pieni ja hoitomuodon pitkäaikaisesta tehosta ei ole riittävästi näyttöä «Transkraniaalinen tasavirtastimulaatio saattaa lievittää ADHD-oireita lumestimulaatiota enemmän välittömästi hoidon jälkeen, mutta vaikutus on pieni ja hoitomuodon pitkäaikaisesta tehosta ei ole riittävästi näyttöä.»D.
- Sarjoittainen magneettistimulaatio (rTMS) ei lievittäne aikuisen ADHD:n oireita kliinisesti merkittävällä tavalla «Repetitive transcranial magnetic stimulation (rTMS) may not alleviate the symptoms of adult ADHD in a clinically meaningful way.»C. Lisäksi on huomioitava, että käytössä olevilla rTMS-laitteilla on viranomaisen hyväksymänä psykiatrisena käyttöaiheena ainoastaan depression hoito.
- Biopalautehoidolla (neurofeedback) ei ilmeisesti ole kliinisesti merkittäviä vaikutuksia lasten «EEG-biopalautehoidolla ei ilmeisesti ole kliinisesti merkittäviä vaikutuksia lasten ja nuorten ADHD-oireisiin.»B tai aikuisten «Biopalautehoidolla ei liene kliinisesti merkittäviä vaikutuksia aikuisten ADHD:n oireisiin.»C ADHD-oireisiin. Tutkimuksia biopalautehoidon vaikutuksista aikuisten ADHD:n oireisiin on tehty huomattavasti vähemmän kuin tutkimuksia sen vaikutuksista lasten oireisiin. Ks. myös Vältä viisaasti -suositus «Biopalautehoito (neurofeedback) ADHD:n hoidossa»68.
- Tietokoneistetulla kognitiivisten taitojen harjoittelulla ei ilmeisesti ole merkittäviä vaikutuksia lasten, nuorten tai aikuisten ADHD:n oireisiin «Tietokoneistetulla kognitiivisten taitojen harjoittelulla ei ilmeisesti ole merkittäviä vaikutuksia lasten, nuorten tai aikuisten ADHD:n oireisiin.»B.
- Homeopatiasta ei ole hyötyä ADHD:n hoidossa «Catalá-López F, Hutton B, Núñez-Beltrán A, ym. The...»201, «Coulter MK, Dean ME. Homeopathy for attention defi...»216, «Rotella F, Cassioli E, Falone A, ym. Homeopathic R...»217.
Ravitsemus
Ravitsemushoidot
- Ravitsemushoidoista on tutkittu tiettyjen ravintoaineiden, kuten rasvahappojen, vitamiinien
ja kivennäisaineiden, lisäämistä ruokavalioon ja niin sanottuja eliminaatioruokavalioita,
joissa ruokavaliosta jätetään pois oireita aiheuttaviksi epäiltyjä ravintoaineita,
ks. lisätietoa «Ravitsemushoidot ja ADHD»69.
- Monityydyttymättömät rasvahapot ovat ilmeisesti tehottomia lasten ja nuorten ADHD:n hoidossa «Monityydyttymättömät rasvahapot ovat ilmeisesti tehottomia ADHD:n hoidossa lapsilla ja nuorilla.»B. Aikuisia koskevaa tutkimustietoa asiasta ei ole. Ks. myös Vältä viisaasti -suositus «Monityydyttymättömät rasvahapot lasten ja nuorten ADHD:n hoidossa»70.
- Lapsen raudanpuuteanemian oireet pitää tutkia ja hoitaa asianmukaisesti, mutta laadukasta
tutkimusnäyttöä rautalisän hyödyllisyydestä ADHD-oireisiin ilman anemiaa ei ole «Panahandeh G, Vatani B, Safavi P, ym. The effect o...»218, «Konofal E, Lecendreux M, Deron J, ym. Effects of i...»219, «Granero R, Pardo-Garrido A, Carpio-Toro IL, ym. Th...»220, «Ryhänen S, Vepsäläinen K, Huurre A, ym. Pienentyny...»221.
- Varastoraudan määrä on joissakin tutkimuksissa ollut ADHD-diagnoosin saaneilla lapsilla ja nuorilla pienempi kuin samanikäisillä verrokeilla «Cortese S, Angriman M, Lecendreux M, ym. Iron and ...»222, «Wang Y, Huang L, Zhang L, ym. Iron Status in Atten...»223. Syynä voivat olla muun muassa stimulanttien ruokahalua heikentävä vaikutus, syömishäiriöt tai ravinnon laatuun liittyvät puutteet.
- ADHD-oireisten lasten varastoraudan todetun vähäisyyden ja runsaan unenaikaisen liikehdinnän välillä saattaa olla yhteyttä «Cortese S, Angriman M, Lecendreux M, ym. Iron and ...»222.
- Magnesiumlisän vaikutuksesta ADHD-oireisiin ei ole riittävästi tutkimustietoa «Hariri M, Azadbakht L. Magnesium, Iron, and Zinc S...»224, «Heilskov Rytter MJ, Andersen LB, Houmann T, ym. Di...»225.
- Ruoka-ainerajoitukset saattavat vähentää joidenkin lasten ja nuorten ADHD-oireita, mutta tutkimusnäyttöä
ei ole riittävästi vaikuttavuuden arvioimiseksi «Ruoka-ainerajoitukset saattavat vähentää joidenkin lasten ja nuorten ADHD-oireita, mutta luotettava näyttö puuttuu.»D.
- Pois jätettävät ruoka-aineet pitäisi valita yksilöllisesti ja vasta sitten, kun oireiden mahdollinen yhteys ruoka-aineisiin on todettu seurantapäiväkirjan avulla.
- Jos eliminaatioruokavalioon päädytään, tarvitaan ravitsemusneuvontaa riittävän monipuolisen ja terveellisen ravinnonsaannin turvaamiseksi.
- Sakkaroosin poistamisella ruokavaliosta ei ilmeisesti ole merkitystä lasten tai nuorten ADHD-oireiden hoidossa «Sakkaroosin poistamisella ruokavaliosta ei ilmeisesti ole merkitystä lasten tai nuorten ADHD-oireiden hoidossa.»B.
- Keinotekoisten lisäaineiden, kuten keinotekoisten väriaineiden ja salisylaattien, poistaminen ruokavaliosta saattaa osalla lapsista vähentää ADHD-oireita, mutta luotettava
näyttö asiasta puuttuu «Keinotekoisten lisäaineiden poistaminen ruokavaliosta saattaa osalla lapsista vähentää ADHD-oireita, mutta luotettava näyttö puuttuu.»D.
- Aspartaami ei vuonna 2020 julkaistun systemaattisen katsauksen mukaan lisää ADHD-oireita «Uldall Torp NM, Thomsen PH. The use of diet interv...»226.
- Suositus 20: Työryhmä ei suosita ravitsemushoitoja ADHD-oireiden lievittämiseen.
Ruokavalio
- Ruokavalion laadun ja ADHD-oireiden yhteydestä on saatavilla ristiriitaista tutkimustietoa. Ruokavalion laadulla voi olla merkitystä ADHD:n riskin kannalta, mutta tämän vahvistamiseksi tarvitaan laajoja satunnaistettuja vertailevia tutkimuksia.
- ADHD-oireisten henkilöiden epäterveellisten ruokatottumusten riski saattaa olla suurentunut ja lääkehoito voi heikentää ruokahalua, minkä vuoksi ravintoaineiden riittävyys ja ruokavalion laatu on tärkeää huomioida osana hoitoa ja seurantaa «Lange KW, Lange KM, Nakamura Y, ym. Nutrition in t...»227, «Shareghfarid E, Sangsefidi ZS, Salehi-Abargouei A,...»228. Tarvittaessa henkilö tulee ohjata ravitsemusterapeutin vastaanotolle.
- Suositus 21: Työryhmä suosittaa kiinnittämään huomiota ateriarytmin säännöllisyyteen ja ruokavalion monipuolisuuteen ADHD-oireisten henkilöiden hyvinvoinnin tukemisessa.
Hoito ADHD:n kanssa samanaikaisesti esiintyvien häiriöiden ja sairauksien yhteydessä
- ADHD:n kanssa esiintyy usein samanaikaisesti muita häiriöitä tai sairauksia. Osalla
niistä lienee samantyyppinen neurobiologinen alkuperä, mutta osa voi kehittyä sekundaarisina,
esimerkiksi reaktiivinen masennus toistuvien epäonnistumisten seurauksena. Psykiatriset
samanaikaishäiriöt myös komplisoivat ADHD:n hoitoa ja lisäävät oppimiseen ja toimintakykyyn
liittyviä ongelmia «Joelsson P, Chudal R, Gyllenberg D, ym. Demographi...»16.
- Suomalaisessa väestöpohjaisessa tutkimuksessa «Joelsson P, Chudal R, Gyllenberg D, ym. Demographi...»16 vuosina 1991–2005 syntyneillä erikoissairaanhoidossa ADHD-diagnoosin saaneilla samanaikaishäiriöiden
esiintyvyys oli 5–20 vuoden iässä 77 %.
- Tavallisimpia olivat kehitykselliset kielihäiriöt, oppimisvaikeudet tai kehityksellinen koordinaatiohäiriö (48 %), uhmakkuus- ja käytöshäiriöt (28 %), ahdistuneisuushäiriöt (14 %), autismikirjon häiriöt (12 %) ja masennus (9 %).
- Useimmat arviot samanaikaishäiriöiden esiintyvyydestä on tehty poikien aineistoilla.
- ADHD-diagnoosin saaneiden tyttöjen uhmakkuus- ja käytöshäiriön, masennuksen ja ahdistuneisuushäiriöiden riski on suurempi kuin verrokkityttöjen «Tung I, Li JJ, Meza JI, ym. Patterns of Comorbidit...»229.
- Tytöillä on enemmän kielellisiä erityisvaikeuksia, ahdistuneisuushäiriöitä ja masennusta kuin pojilla «Joelsson P, Chudal R, Gyllenberg D, ym. Demographi...»16.
- Aikuisilla samanaikaisia häiriöitä on esiintynyt 50–87 %:lla «Fayyad J, Sampson NA, Hwang I, ym. The descriptive...»9.
- Riski sekä mieliala- että ahdistuneisuushäiriöihin on 3–5-kertainen muuhun väestöön verrattuna «Wymbs BT, Canu WH, Sacchetti GM, ym. Adult ADHD an...»174.
- Suomalaisessa väestöpohjaisessa tutkimuksessa «Joelsson P, Chudal R, Gyllenberg D, ym. Demographi...»16 vuosina 1991–2005 syntyneillä erikoissairaanhoidossa ADHD-diagnoosin saaneilla samanaikaishäiriöiden
esiintyvyys oli 5–20 vuoden iässä 77 %.
- Kun henkilöllä on useita samanaikaisia häiriöitä, hoito yleensä aloitetaan toimintakykyä
eniten haittaavasta tai vakavampioireisesta häiriöstä. ADHD-oireiden hyvä hoito voi
tehostaa myös samanaikaisen häiriön hoidosta hyötymistä «Eom TH, Kim YH. Clinical practice guidelines for a...»121, «AADPA. Australian Evidence-Based Clinical Practice...»124, «Zeanah CH, Chesher T, Boris NW, ym. Practice Param...»230. Kompleksisen ADHD:n hoidon algoritmikaavioita on esitetty artikkelissa «Barbaresi WJ, Campbell L, Diekroger EA, ym. The So...»123.
- ADHD:n psykososiaalisia hoito- ja kuntoutusmenetelmiä voi toteuttaa, vaikka henkilöllä
olisi muu ensisijaisesti hoidettava sairaus. Useimpia menetelmistä käytetään myös
muiden neurokehityksellisten häiriöiden kuntoutuksessa.
- Vanhemmuustaito-ohjaus ja käyttäytymisen ohjaukseen perustuvat menetelmät ovat näyttöön perustuvaa hoitoa muun muassa autismikirjon häiriön ja käytöshäiriöiden hoidossa. Ks. Käypä hoito -suositukset Autismikirjon häiriö «Autismikirjon häiriö»9, «Autismikirjon häiriö. Käypä hoito -suositus. Suoma...»140 ja Käytöshäiriöt (lapset ja nuoret) «Käytöshäiriöt (lapset ja nuoret)»10, «Käytöshäiriöt (lapset ja nuoret). Käypä hoito -suo...»141.
- Lääkehoidossa on otettava huomioon lääkkeiden mahdolliset yhteisvaikutukset sekä somaattiset sairaudet, kuten sydän- ja verisuonisairaudet, joihin ADHD:n lääkehoito voi vaikuttaa.
- ADHD:n psykososiaalisia hoito- ja kuntoutusmenetelmiä voi toteuttaa, vaikka henkilöllä
olisi muu ensisijaisesti hoidettava sairaus. Useimpia menetelmistä käytetään myös
muiden neurokehityksellisten häiriöiden kuntoutuksessa.
- Suositus 22: Työryhmä suosittaa ottamaan samanaikaiset häiriöt huomioon hoidossa ja kuntoutusmenetelmien valinnassa.
Keskeisimmät samanaikaiset neurokehitykselliset oireyhtymät
- Hieno- ja karkeamotoriikan sekä aistitiedon käsittelyn vaikeuksia esiintyy eri tutkimusten mukaan 30–80 %:lla ADHD-diagnoosin saaneista lapsista «Kirby A, Salmon G, Edward L. Should Children with ...»231, «Raynolds F. Occupational Therapy for Children with...»232, «Kaiser ML, Schoemaker MM, Albaret JM, ym. What is ...»233, «Goulardins JB, Rigoli D, Licari M, ym. Attention d...»234, «Dellapiazza F, Michelon C, Vernhet C, ym. Sensory ...»235, (ks. lisätietoa Aistitiedon käsittelyn ja säätelyn häiriöt «Aistitiedon käsittelyn vaikeudet ja ADHD»60). Motoriikan ja aistitiedon käsittelyn ongelmat jatkuvat usein nuoruuteen ja aikuisuuteen
«Stray LL, Kristensen Ø, Lomeland M, ym. Motor regu...»236, «Kamath MS, Dahm CR, Tucker JR, ym. Sensory profile...»237, «Adra N, Cao A, Makris N, ym. Sensory Modulation Di...»238, «Hyde C, Fuelscher I, Efron D, ym. Adolescents with...»239. ADHD-oireet voivat haitata esimerkiksi hienomotorista pikkutarkkuutta vaativaa työskentelyä.
- Lasten ja nuorten kehityksellisen koordinaatiohäiriön (DCD) Käypä hoito -suosituksen
mukaan «Lasten ja nuorten kehityksellinen koordinaatiohäiriö (DCD)»8, «Lasten ja nuorten kehityksellinen koordinaatiohäir...»139
- metyylifenidaatti saattaa parantaa motorista suoriutumista, hienomotoriikkaa «Metyylifenidaatti saattaa parantaa motorista suoriutumista lapsilla, joilla on todettu sekä kehityksellinen koordinaatiohäiriö (DCD) että aktiivisuuden ja tarkkaavuuden häiriö (ADHD).»C ja käsialaa «Metyylifenidaatti saattaa parantaa hienomotoriikkaa ja käsin kirjoittamisen tarkkuutta lumelääkkeeseen verrattuna lapsilla, joilla on sekä kehityksellinen koordinaatiohäiriö (DCD) että aktiivisuuden ja tarkkaavuuden häiriö (ADHD), mutta luotettava näyttö puuttuu.»D lapsilla, joilla on sekä ADHD että DCD, sekä vaikuttaa positiivisesti elämänlaatuun «Metyylifenidaatti saattaa parantaa elämänlaatua lapsilla, joilla on todettu sekä kehityksellinen koordinaatiohäiriö (DCD) että aktiivisuuden ja tarkkaavuuden häiriö (ADHD), mutta luotettava näyttö puuttuu.»D, mutta luotettava näyttö puuttuu
- lääkehoito ei yksinään riitä parantamaan motorisia taitoja, vaan lisäksi tarvitaan muita tukitoimia ja kuntoutusta.
- Lasten ja nuorten kehityksellisen koordinaatiohäiriön (DCD) Käypä hoito -suosituksen
mukaan «Lasten ja nuorten kehityksellinen koordinaatiohäiriö (DCD)»8, «Lasten ja nuorten kehityksellinen koordinaatiohäir...»139
- Puheen ja kielen kehityksen häiriöiden riski on ADHD-oireisilla lapsilla jopa kolminkertainen, mutta arviot kehityksellisen kielihäiriön
ja ADHD:n samanaikaisuudesta kuitenkin vaihtelevat «Mueller KL, Tomblin JB. Examining the comorbidity ...»240, «Sciberras E, Mueller KL, Efron D, ym. Language pro...»241, «Carruthers S, Taylor L, Sadiq H, ym. The profile o...»242, «Korrel H, Mueller KL, Silk T, ym. Research Review:...»243, «Méndez-Freije I, Areces D, Rodríguez C. Language S...»244.
- Kaksi yleisintä kielen kehitykseen vaikuttavaa kehityksellistä häiriötä ovat ADHD ja kehityksellinen kielihäiriö (DLD, developmental language disorder). Kielen kehityksellä on olennainen merkitys kognitiiviselle ja sosiaaliselle kehitykselle. Kielellisten taitojen haasteet voivat vaikuttaa epäedullisesti muun muassa sosiaaliseen vuorovaikutukseen «Parks KMA, Hannah KE, Moreau CN, ym. Language abil...»245.
- ADHD:n kanssa samanaikaisen kehityksellisen kielihäiriön kuntoutus toteutetaan sitä koskevan Käypä hoito -suosituksen mukaisesti, ks. Käypä hoito -suositus Kehityksellinen kielihäiriö (kielellinen erityisvaikeus, lapset ja nuoret) «Kehityksellinen kielihäiriö (kielellinen erityisvaikeus, lapset ja nuoret)»7, «Kehityksellinen kielihäiriö (kielen kehityksen häi...»138.
- Erityiset oppimisvaikeudet (ks. lisätietoa «Oppimisvaikeudet ja ADHD»38) ovat tavallisempia ADHD-diagnoosin saaneilla kuin verrokeilla «Frazier TW, Youngstrom EA, Glutting JJ, ym. ADHD a...»246, «Sexton CC, Gelhorn HL, Bell JA, ym. The co-occurre...»247, «DuPaul GJ, Gormley MJ, Laracy SD. Comorbidity of L...»248, «Barkley R, Murphy KR, Fischer M. ADHD in adults: w...»249, «Tervo T, Michelsson K, Launes J, ym. A Prospective...»250, ja ne voivat merkittävästi vaikeuttaa suoriutumista koulussa ja perusopetuksen jälkeisessä
koulutuksessa «Taanila A, Ebeling H, Tiihala M, ym. Association b...»251 sekä myöhemmin myös työelämässä.
- Koska ADHD:n ydinoireita vähentävät hoidot eivät ilmeisesti juuri vaikuta lukemisen ja matematiikan taitojen kehittymiseen, mahdollisiin oppimisvaikeuksin tulee suunnitella riittävät tukitoimet ja tarvittava kuntoutus (ks. lisätietoa «ADHD-hoitojen vaikutus opilliseen suoriutumiseen koulussa»71.
- Autismikirjon häiriön (autism spectrum disorder, ASD) (ks. Käypä hoito -suositus Autismikirjon häiriö
«Autismikirjon häiriö»9, «Autismikirjon häiriö. Käypä hoito -suositus. Suoma...»140) yhteydessä esiintyvän ADHD:n esiintyvyydeksi lapsilla on arvioitu 30–80 % «Leyfer OT, Folstein SE, Bacalman S, ym. Comorbid p...»252, «Rommelse NN, Franke B, Geurts HM, ym. Shared herit...»253. ADHD:n yhteydessä samanaikaisia autismikirjon häiriön piirteitä taas on arvioitu
esiintyvän 20–50 %:lla lapsista «Leyfer OT, Folstein SE, Bacalman S, ym. Comorbid p...»252. Aikuisilla ADHD:n esiintymistä samanaikaisesti autismikirjon häiriöiden kanssa on
tutkittu vain vähän. Yhteys näyttää heikkenevän varsin voimakkaasti, mitä vanhempaa
ikäryhmää tutkitaan «Supekar K, Iyer T, Menon V. The influence of sex a...»254, «Hartman CA, Geurts HM, Franke B, ym. Changing ASD-...»255.
- Merkittävän samanaikaisuuden vuoksi on suositeltavaa kaikissa ikäryhmissä arvioida
sekä ADHD:n että autismikirjon häiriön mahdollisuutta osana diagnostista prosessia.
- Toiminnanohjauksen vaikeudet ovat tyypillisiä molemmissa häiriöissä.
- Autismikirjon häiriössä erityisesti toimintojen suunnittelu ja joustavuus ovat puutteellisia, kun taas ADHD:ssä tyypillisempiä ovat inhibitoriset vaikeudet, tarkkaavuuden ylläpitämisen vaikeudet ja työmuistin kapeus.
- Oirekuvien osittaisen päällekkäisyyden vuoksi kehityksellisten häiriöiden erottaminen toisistaan ei aina ole helppoa.
- Samanaikaisen ADHD:n hoito ja kuntoutus on tärkeää, koska joidenkin tutkimusten mukaan ADHD:n ja autismikirjon samanaikainen esiintyminen voi lisätä muun samanaikaissairastavuuden riskiä.
- ADHD:n ja ASD:n esiintyessä samanaikaisesti käytetään ensisijaisesti psykososiaalisia
hoitomuotoja, kuten käyttäytymishoitoa ja sen sovelluksia eri ympäristöissä.
- Myös ympäristön muokkauksessa tulisi huomioida molempien häiriöiden erityispiirteet ja tarpeet.
- ADHD:n lääkehoitoa on syytä kokeilla, jos lääkkeetön hoito ei ole riittävä ja tarkkaamattomuus,
ylivilkkaus tai impulsiivisuus aiheuttavat selvää haittaa.
- Stimulanteista ja atomoksetiinista voi olla hyötyä ADHD-oireiden lievittämisessä henkilöillä, joilla on autismikirjon häiriö «Ji N, Findling RL. An update on pharmacotherapy fo...»256, «Beherec L, Quilici G, Rosier A, Gerardin P, Campio...»257, «Baribeau DA, Anagnostou E. An update on medication...»258 «Reichow B, Volkmar FR, Bloch MH. Systematic review...»259, «Scahill L, McCracken JT, King BH, ym. Extended-Rel...»260.
- Tarkka seuranta sopivan annostelun etsimisen yhteydessä lääkkeen aloitusvaiheessa on välttämätöntä, sillä henkilöt, joilla on samanaikainen autismikirjon häiriö, näyttävät olevan herkempiä ADHD-lääkkeiden haittavaikutuksille «Mahajan R, Bernal MP, Panzer R, ym. Clinical pract...»261.
- Merkittävän samanaikaisuuden vuoksi on suositeltavaa kaikissa ikäryhmissä arvioida
sekä ADHD:n että autismikirjon häiriön mahdollisuutta osana diagnostista prosessia.
- Tic-oireita (ks. lisätietoa «Tic-häiriöt ja ADHD»72) esiintyy noin 20–30 %:lla ADHD-oireisista lapsista «Hirschtritt ME, Lee PC, Pauls DL, ym. Lifetime pre...»262.
- Jos esiintyy pitkäkestoisia samanaikaisia motorisia ja vokaalisia tic-oireita, kyseessä
on Touretten oireyhtymä «Puustjärvi A, Raaska H. Tourette oireyhtymä ja muu...»263. Sen esiintyvyys on lapsuus- ja nuoruusiässä pojilla noin 1,0 % ja tytöillä noin
0,3 % «Hirschtritt ME, Lee PC, Pauls DL, ym. Lifetime pre...»262. Tic-oireiden ja Touretten oireyhtymän hoidossa ensisijaisia ovat kognitiivis-behavioraaliset
menetelmät «Andrén P, Jakubovski E, Murphy TL, ym. European cl...»264
- ADHD on Touretten oireyhtymän tavallisin samanaikaishäiriö (50–60 %:lla) «Hirschtritt ME, Lee PC, Pauls DL, ym. Lifetime pre...»262, «Johnson KA, Worbe Y, Foote KD, ym. Tourette syndro...»265
- Touretten oireyhtymää sairastavilla ADHD heikentää toimintakykyä jopa enemmän kuin tic-oireet. Se heikentää myös psykososiaalista selviytymistä ja elämänlaatua usein aikuisikään asti «Hirschtritt ME, Lee PC, Pauls DL, ym. Lifetime pre...»262, «Johnson KA, Worbe Y, Foote KD, ym. Tourette syndro...»265
- ADHD:n asianmukainen ja onnistunut hoito näyttää vähentävän myös tic-oireita «Johnson KA, Worbe Y, Foote KD, ym. Tourette syndro...»265, «Roessner V, Eichele H, Stern JS, ym. European clin...»266.
- Kaikki Suomessa hyväksytyt ADHD-lääkkeet ovat tehokkaita myös Touretten oireyhtymän yhteydessä «Roessner V, Eichele H, Stern JS, ym. European clin...»266, «Osland ST, Steeves TD, Pringsheim T. Pharmacologic...»267.
- Psykostimulantit voivat voimistaa tic-oireita, mutta näin käy tutkimusten mukaan harvoin, eivätkä tic-oireet tai Touretten oireyhtymä ole psykostimulanttien käytön vasta-aihe «Roessner V, Eichele H, Stern JS, ym. European clin...»266, «Osland ST, Steeves TD, Pringsheim T. Pharmacologic...»267.
- Muista ADHD-lääkkeistä alfa2-agonisti guanfasiinilla on todettu olevan suotuisin vaste samanaikaisesti esiintyviin tic- ja ADHD-oireisiin «Roessner V, Eichele H, Stern JS, ym. European clin...»266, «Osland ST, Steeves TD, Pringsheim T. Pharmacologic...»267.
- Jos esiintyy pitkäkestoisia samanaikaisia motorisia ja vokaalisia tic-oireita, kyseessä
on Touretten oireyhtymä «Puustjärvi A, Raaska H. Tourette oireyhtymä ja muu...»263. Sen esiintyvyys on lapsuus- ja nuoruusiässä pojilla noin 1,0 % ja tytöillä noin
0,3 % «Hirschtritt ME, Lee PC, Pauls DL, ym. Lifetime pre...»262. Tic-oireiden ja Touretten oireyhtymän hoidossa ensisijaisia ovat kognitiivis-behavioraaliset
menetelmät «Andrén P, Jakubovski E, Murphy TL, ym. European cl...»264
Keskeisimmät neurologiset ja somaattiset samanaikaishäiriöt
- Unihäiriöt ovat sekä subjektiivisen raportoinnin että objektiivisten unitutkimusten mukaan ADHD-diagnoosin
saaneilla yleisiä «Cortese S, Faraone SV, Konofal E, ym. Sleep in chi...»268, «Bondopadhyay U, Diaz-Orueta U, Coogan AN. A System...»269, «Martins R, Scalco JC, Ferrari Junior GJ, ym. Sleep...»270, «Arias-Mera C, Paillama-Raimán D, Lucero-González N...»271, (ks. myös Käypä hoito -suositus Unettomuus «Unettomuus»20, «Unettomuus. Käypä hoito -suositus. Suomalaisen Lää...»272).
- Unihäiriöiden mahdolliset syyt tulee selvittää unianamneesin (unen huolto, nukkumisolot, älylaitteiden käyttö) ja tarvittaessa objektiivisten unitutkimusten avulla. Erilaiset muut uneen ja nukkumiseen vaikuttavat unihäiriöt, kuten viivästynyt unijakso, levottomien jalkojen oireyhtymä, uniapnea ja narkolepsia tulee ottaa huomioon.
- ADHD-lääkitys voi vaikeuttaa nukahtamista illalla, mutta joskus myös parantaa (etenkin aikuisten) unen laatua «Sobanski E, Schredl M, Kettler N, ym. Sleep in adu...»273.
- Unenhuoltoa parantavat toimet (säännöllinen unirytmi, iltarituaalit, älylaitteiden
käytön rajoittaminen illalla ja yöllä jne.) ovat ensisijaisia kaikilla, joilla on
univaikeuksia «Paavonen J, Sarvasmaa AS. Unihäiriöt. Kirjassa: La...»274, «Larsson I, Aili K, Lönn M, ym. Sleep interventions...»275, «Malkani MK, Pestell CF, Sheridan AMC, ym. Behavior...»276, (ks. lisätietoa «Unihäiriöt ja ADHD»73).
- Melatoniini saattaa lyhentää sellaisten stimulanttilääkitystä saavien lasten tai nuorten nukahtamisaikaa, joille pelkät unenhuoltoa parantavat toimet tai ADHD:n lääkehoidon säätö eivät ole riittäviä «Weiss MD, Wasdell MB, Bomben MM, ym. Sleep hygiene...»277, «Van der Heijden KB, Smits MG, Van Someren EJ, ym. ...»278 Melatoniinista saattaa olla apua myös aikuisten ADHD:hen liittyvien univaikeuksien lievittämisessä «Coogan AN, McGowan NM. A systematic review of circ...»279, «Parvataneni T, Srinivas S, Shah K, ym. Perspective...»280. Tutkimustietoa melatoniinin pitkäaikaisesta käytöstä ADHD:n hoidon yhteydessä ei ole.
- Epilepsiaa sairastavilla on todettu enemmän ADHD:tä kuin väestöllä yleensä, ja ADHD-diagnoosin
saaneilla on enemmän epilepsiaa kuin muulla väestöllä «Wang S, Yao B, Zhang H, ym. Comorbidity of epileps...»281, «Ono KE, Bearden DJ, Lee SM, ym. Interventions for ...»282, «Rheims S, Auvin S. Attention deficit/hyperactivity...»283, «Fan HC, Chiang KL, Chang KH, ym. Epilepsy and Atte...»284. Samanaikainen, kahdensuuntainen suurentunut esiintyvyys viittaa siihen, että epilepsialla
ja ADHD:llä ei ole syy-seuraussuhdetta keskenään, vaan niiden taustalla on yhteisiä
syytekijöitä, ks. lisätietoa «Epilepsia ADHD:n samanaikaissairautena ja erotusdiagnostiikassa»37.
- Epilepsia ei ole este ADHD:n tehokkaalle hoidolle. Epilepsiaa sairastavan lapsen ADHD:tä tulisi hoitaa aktiivisesti «Reilly CJ. Attention deficit hyperactivity disorde...»285, ks. lisätietoa «Epilepsiaa sairastavan lapsen ADHD-oireiden hoito»74.
- Epilepsiaa sairastavien ADHD:n diagnostiikka ja hoito toteutetaan samojen periaatteiden ja hoidon porrastuksen mukaisesti kuin muun väestön ADHD:n hoito. Epilepsiaa sairastavien keskittymisen ja tarkkaavuuden ongelmista osa voi johtua kohtauksista tai liittyä epilepsian lääkehoitoon «Ono KE, Bearden DJ, Lee SM, ym. Interventions for ...»282.
- Epilepsiaa sairastavien ADHD:n lääkehoito on osoitettu turvalliseksi tavanomaisilla ADHD:n hoitoon käytetyillä annoksilla «Wang S, Yao B, Zhang H, ym. Comorbidity of epileps...»281, «Ono KE, Bearden DJ, Lee SM, ym. Interventions for ...»282, «Rheims S, Auvin S. Attention deficit/hyperactivity...»283. Isoissa aineistoissa sen ei ole osoitettu lisäävän kohtausten määrää «Brikell I, Chen Q, Kuja-Halkola R, ym. Medication ...»286, «Wiggs KK, Chang Z, Quinn PD, ym. Attention-deficit...»287.
- Jos epäillään ADHD-lääkityksen aiheuttavan tai lisäävän epileptisiä kohtauksia, on tilanne arvioitava yksilöllisesti huomioiden mahdolliset muut kohtauksia provosoivat tekijät. ADHD-lääkitykseen ei tarvitse tehdä automaattisesti muutoksia.
- Käsitys kehitysvammaisten lasten ADHD:stä on muuttunut, kun kognitiivinen taso ja profiili ovat tulleet paremmin
ymmärretyiksi neuropsykologisen tutkimuksen myötä. Aiemmin ADHD-diagnoosin oikeutusta
kehitysvammaisilla epäröitiin «Antshel KM, Phillips MH, Gordon M, ym. Is ADHD a v...»288, «Deutsch CK, Dube WV, McIlvane WJ. Attention defici...»289. Nykytietämyksen mukaan kehitysvammaisilla on enemmän ADHD:tä kuin muulla väestöllä
«Li Q, Li Y, Zheng J, ym. Prevalence and trends of ...»290, «Perera B, Chen J, Korb L, ym. Patterns of comorbid...»291
- Kehitysvammaisten lasten ADHD-oireiden arvioinnissa olennaisin menetelmä on kehitysvammaisten hoitoon perehtyneiden ammattilaisten kliininen arvio «Freeman NC, Gray KM, Taffe JR, ym. Development of ...»292, «Freeman NC, Gray KM, Taffe JR, ym. A cross-syndrom...»293, «Perera B, Courtenay K, Solomou S, ym. Diagnosis of...»294. Pelkästään muulle väestölle suunnattujen kyselylomakkeiden käyttö näyttää johtavan ylidiagnostiikkaan ja väärin kohdistuviin diagnooseihin «Arias VB, Arias B, Burns GL, ym. Invariance of par...»295, «Sun CK, Tseng PT, Wu CK, ym. Therapeutic effects o...»296.
- Kehitysvammaisten ADHD:n hoito toteutetaan kuten muidenkin ADHD-diagnoosin saaneiden.
- Osa ADHD-oireisista kehitysvammaisista hyötyy ADHD:n lääkehoidosta, eikä ainakaan metyylifenidaatista näyttäisi aiheutuvan kehitysvammaisille enempää haittavaikutuksia kuin kognitiivisesti keskitasoisille, mutta hyötyjen ja haittojen seuraaminen saattaa olla vaikeampaa «Perera B, Chen J, Korb L, ym. Patterns of comorbid...»291, «Sun CK, Tseng PT, Wu CK, ym. Therapeutic effects o...»296, «Tarrant N, Roy M, Deb S, ym. The effectiveness of ...»297.
Keskeisimmät psykiatriset samanaikaishäiriöt
- Käytöshäiriö on lapsilla ja nuorilla tavallisin ADHD:n kanssa samanaikaisesti esiintyvä psykiatrinen
häiriö «Thapar A, Cooper M. Attention deficit hyperactivit...»33, (ks. lisätietoa «Käytöshäiriöt ja ADHD»39 sekä Käypä hoito -suositus Käytöshäiriöt (lapset ja nuoret) «Käytöshäiriöt (lapset ja nuoret)»10, «Käytöshäiriöt (lapset ja nuoret). Käypä hoito -suo...»141).
- Noin 10–40 % ADHD-diagnoosin saaneista lapsista ja nuorista täyttää samanaikaisesti käytöshäiriön kriteerit «Tung I, Li JJ, Meza JI, ym. Patterns of Comorbidit...»229, «Osland ST, Steeves TD, Pringsheim T. Pharmacologic...»267, «Tesli N, Jaholkowski P, Haukvik UK, ym. Conduct di...»298.
- Samanaikaisen ADHD:n ja käytöshäiriön kliinisessä kuvassa korostuvat yliaktiivisuus- ja impulsiivisuusoireet, sosiaaliset vaikeudet ja lapsen ja vanhempien huono suhde «Connor DF, Steeber J, McBurnett K. A review of att...»299.
- Samanaikainen uhmakkuus- tai käytöshäiriö heikentää ADHD-diagnoosin saaneen lapsen
tai nuoren toimintakykyä ja ADHD:n pitkäaikaisennustetta ja aiheuttaa noin kaksinkertaisen
riskin ADHD-oireiden jatkumiselle merkittävinä aikuisikään «Caye A, Spadini AV, Karam RG, ym. Predictors of pe...»300.
- Molemmat häiriöt vaikuttavat paljon toimintakykyyn perheessä, koulussa ja ikätoverisuhteissa ja altistavat sekä psyykkisten että psykososiaalisten lisäongelmien kehittymiselle.
- ADHD:n ja samanaikaisen käytöshäiriön varhainen diagnostiikka ja aktiivinen hoito ovat erittäin tärkeitä. Monimuotoinen hoito, joka sisältää ikäryhmälle sopivia psykososiaalisia hoitokeinoja (esim. strukturoidun vanhempainohjauksen, lapsen ja nuoren sosiaalisten ja tunnetaitojen tukemisen) ja ADHD:n lääkehoidon, on usein tarpeen.
- Psykostimulanttien, atomoksetiinin ja guanfasiinin on todettu vähentävän myös käytöshäiriöoireita ADHD-diagnoosin saaneilla lapsilla «Gurnani T, Ivanov I, Newcorn JH. Pharmacotherapy o...»301.
- ADHD ja kiintymyssuhdehäiriö (ks. lisätietoa «Lapsuuden kiintymyssuhdehäiriöt ja ADHD»40) ovat erotettavissa toisistaan huolellisella esitietoihin ja ydinoireisiin kohdentuvalla
diagnostiikalla.
- Kiintymyssuhdehäiriön diagnoosi edellyttää lapsen historiassa olevan varmaa tai todennäköistä ja vakavaa hoivan puutteellisuutta «The World Health Organization (WHO). International...»130.
- Sekä ADHD:n että kiintymyssuhdehäiriöiden on todettu lisäävän nuoruus- ja aikuisikäisten psykososiaalisten vaikeuksien riskiä. Sen vuoksi molempien häiriöiden tunnistaminen ja yhtäaikainen hoito on tärkeää.
- Kiintymyssuhdehäiriön kanssa samanaikaisen ADHD:n hoito suositellaan toteutettavan ADHD:n hoitosuosituksen mukaisesti kiinnittäen kuitenkin erityistä huomiota lapsen ja vanhemman välisen suhteen tukemiseen «Zeanah CH, Chesher T, Boris NW, ym. Practice Param...»230.
- ADHD:n ja traumaperäisen stressihäiriön (posttraumatic stress disorder, PTSD) (ks. lisätietoa «ADHD ja traumaperäiset häiriöt»42) oireissa on päällekkäisyyttä, ja ne myös esiintyvät usein samanaikaisesti «Aronen E, Takala L, Haravuori H. Traumaperäiset st...»302, «Koenen KC, Moffitt TE, Poulton R, ym. Early childh...»303, «Spencer AE, Faraone SV, Bogucki OE, ym. Examining ...»304, «Antshel KM, Kaul P, Biederman J, ym. Posttraumatic...»305. Ks. myös Käypä hoito -suositus Traumaperäinen stressihäiriö «Traumaperäinen stressihäiriö»15, «Traumaperäinen stressihäiriö. Käypä hoito -suositu...»146.
- Traumakokemukset voivat voimistaa ADHD-oireita «Aronen E, Takala L, Haravuori H. Traumaperäiset st...»302, «Harrington KM, Miller MW, Wolf EJ, ym. Attention-d...»306, ja ADHD voi vahvistaa traumaperäisen stressihäiriön oireita «Martínez L, Prada E, Satler C, ym. Executive Dysfu...»307, «Zhang N, Gao M, Yu J, ym. Understanding the associ...»308.
- ADHD voi lisätä alttiutta myöhemmille traumakokemuksille, kaltoinkohtelulle ja niiden aiheuttamille psyykkisille häiriöille «Koenen KC, Moffitt TE, Poulton R, ym. Early childh...»303, «Adler LA, Kunz M, Chua HC, ym. Attention-deficit/h...»309.
- Pakolaisilla, sijoitetuilla tai seksuaalisesti hyväksikäytetyillä lapsilla ja nuorilla ADHD:n esiintyminen näyttää olevan yleisempää kuin muilla «Penttilä S, Niemelä M, Hakko H, ym. Child- and par...»125, «Lehti V, Chudal R, Suominen A, ym. Association bet...»126, «Klein B, Damiani-Taraba G, Koster A, ym. Diagnosin...»310, «Daud A, Rydelius PA. Comorbidity/overlapping betwe...»311, «Weinstein D, Staffelbach D, Biaggio M. Attention-d...»312, «Blackmore R, Gray KM, Boyle JA, ym. Systematic Rev...»313.
- Traumatisoivat kokemukset, kuten kaltoinkohtelu tai laiminlyönti lapsuudessa ja perhe-
tai muu väkivalta, tulee selvittää ADHD-oireiden arvioinnin ja hoitosuunnitelman teon
yhteydessä.
- Jos lapsella todetaan samanaikainen traumaperäinen stressihäiriö, ADHD-oireita on arvioitava uudestaan viimeistään silloin, kun traumaan liittyvä oireilu on lievittynyt «AADPA. Australian Evidence-Based Clinical Practice...»124, «Klein B, Damiani-Taraba G, Koster A, ym. Diagnosin...»310.
- Samanaikaisen traumaperäisen häiriön ja ADHD:n hoito on suunniteltava yksilöllisesti, ja siinä tarvitaan usein sekä PTSD:n että ADHD:n ikäryhmäkohtaisia psykososiaalisia hoitomuotoja, mahdollisesti myös toisen tai molempien häiriöiden lääkehoitoa (nuorilla ja aikuisilla). Näyttöä lasten PTSD:n lääkehoidosta ei ole, ks. Käypä hoito -suositus Traumaperäinen stressihäiriö «Traumaperäinen stressihäiriö»15, «Traumaperäinen stressihäiriö. Käypä hoito -suositu...»146.
- Guanfasiinin ja klonidiinin on arveltu olevan soveltuvimpia ADHD:n hoitoon samanaikaisen traumaperäisen stressihäiriön yhteydessä, mutta tutkimustietoa aiheesta on toistaiseksi niukasti «Belkin MR, Schwartz TL. Alpha-2 receptor agonists ...»314, «Lee DJ, Schnitzlein CW, Wolf JP, ym. PSYCHOTHERAPY...»315, «Jagtiani A, Gandhi R, Banga A, ym. Alpha-2 Agonist...»316. Soveltuvuuden perusteluna on käytetty näiden lääkkeiden verenpainetta ja pulssia laskevaa vaikutusta, jonka on ajateltu epäsuorasti voivan lievittää myös traumaperäiseen stressihäiriöön liittyvää pitkittynyttä vireystilan nousua.
- Ahdistuneisuushäiriöitä esiintyy 15–50 %:lla lapsista ja nuorista, joilla on ADHD «Njardvik U, Wergeland GJ, Riise EN, ym. Psychiatri...»317, «Angold A, Costello EJ, Erkanli A. Comorbidity. J C...»318, «Steinhausen HC, Nøvik TS, Baldursson G, ym. Co-exi...»319, kun ahdistuneisuushäiriöiden esiintyvyys lapsuusiässä on yleisesti 3–9 % ja nuoruusiässä
10–15 % «Ranta K, Koskinen M. Ahdistuneisuushäiriöt. Kirjas...»320. ADHD-diagnoosin saaneista aikuisista jokin ahdistuneisuushäiriö voi olla jopa puolella
«Wymbs BT, Canu WH, Sacchetti GM, ym. Adult ADHD an...»174. Nuorista ja aikuisista, joilla on sosiaalisten tilanteiden pelko, jopa 72 %:lla
voi olla myös ADHD «Jakobsson Støre S, Van Zalk N, Granander Schwartz ...»321. Esiintyvyysluvuissa on kuitenkin suuria eroja tutkimusten välillä.
- Ahdistuneisuus näyttää olevan tavallisinta tarkkaamattomuuspainotteisessa ADHD:ssä «Jakobsson Støre S, Van Zalk N, Granander Schwartz ...»321, «Schatz DB, Rostain AL. ADHD with comorbid anxiety:...»322.
- Ahdistuneisuushäiriöiden ja ADHD:n oireiden päällekkäisyys tulee ottaa huomioon erotusdiagnostiikassa.
- Ahdistuneisuus voi ilmetä myös impulsiivisena toimintana ahdistavissa tilanteissa «Jakobsson Støre S, Van Zalk N, Granander Schwartz ...»321.
- Ahdistuneisuushäiriön ja ADHD:n samanaikainen esiintyminen voimistaa ADHD-oireiden
aiheuttamaa haittaa ja heikentää yleensä huomattavasti sosiaalista toimintakykyä.
Siihen liittyy myös useammin heikkoa kognitiivista suoriutumista ja huonoa itsetuntoa
kuin pelkkään ADHD:hen «Jakobsson Støre S, Van Zalk N, Granander Schwartz ...»321, «Schatz DB, Rostain AL. ADHD with comorbid anxiety:...»322.
- Jos henkilöllä todetaan ADHD tai ahdistuneisuushäiriö, tulee myös toisen häiriön mahdollisuutta arvioida aktiivisesti erityisesti, jos toteutunut hoito ei tuota toivottua vastetta «Jakobsson Støre S, Van Zalk N, Granander Schwartz ...»321.
- Samanaikaisen ADHD:n ja ahdistuneisuuden hoidossa ensisijaisia ovat psykososiaaliset
hoitomuodot kuten psykoterapia, vaikeissa oireissa myös lääkehoito (ADHD:hen tai ahdistukseen)
voi olla tarpeen «Njardvik U, Wergeland GJ, Riise EN, ym. Psychiatri...»317, «Manassis K. When attention-deficit/hyperactivity d...»323, «León-Barriera R, Ortegon RS, Chaplin MM, ym. Treat...»324, ks. myös Käypä hoito -suositukset Ahdistuneisuushäiriöt «Ahdistuneisuushäiriöt»11, «Ahdistuneisuushäiriöt. Käypä hoito -suositus. Suom...»142 ja Pakko-oireinen häiriö (OCD) «Pakko-oireinen häiriö (OCD)»12, «Pakko-oireinen häiriö. Käypä hoito -suositus. Suom...»143.
- Ahdistuneisuushäiriö ei heikennä psykostimulanttien vaikutusta ADHD:n keskeisiin oireisiin «Njardvik U, Wergeland GJ, Riise EN, ym. Psychiatri...»317, «León-Barriera R, Ortegon RS, Chaplin MM, ym. Treat...»324.
- ADHD-lääkkeiden haittavaikutuksena kuvataan ahdistuneisuutta, mutta meta-analyysissä yhteyttä lasten ja nuorten ADHD:n lääkehoidon ja ahdistuksen välillä ei löytynyt «Bryant A, Schlesinger H, Sideri A, ym. A meta-anal...»325.
- Kaikkien syömishäiriöiden riski on suurentunut etenkin naisilla ja tytöillä, joilla on ADHD «Yao S, Kuja-Halkola R, Martin J, ym. Associations ...»326, «Villa FM, Crippa A, Rosi E, ym. ADHD and eating di...»327. Ks. lisätietoa «Syömishäiriöriski ADHD-diagnoosin saaneilla»75.
- ADHD-oireet tai diagnosoitu ADHD liittyvät useiden tutkimusten mukaan ylipainoon, lihavuuteen ja ahmintaoireiluun «Waring ME, Lapane KL. Overweight in children and a...»328, «Mikami AY, Hinshaw SP, Arnold LE, ym. Bulimia nerv...»329, «Cortese S, Isnard P, Frelut ML, ym. Association be...»330, ks. myös lisätietoa «Syömishäiriöt ja ADHD»76.
- Syömishäiriöitä sairastavilla on ilmeisesti enemmän ADHD:tä verrattuna muihin samanikäisiin «Syömishäiriöitä sairastavilla on ilmeisesti enemmän ADHD:tä verrattuna muihin samanikäisiin.»B.
- Ks. myös Käypä hoito -suositukset Lihavuus (lapset, nuoret ja aikuiset) «Lihavuus (lapset, nuoret ja aikuiset)»21, «Lihavuus (lapset, nuoret ja aikuiset). Käypä hoito...»331 ja Syömishäiriöt «Syömishäiriöt»22 «Syömishäiriöt. Käypä hoito -suositus. Suomalaisen ...»332
- Masennusta esiintyy samanaikaisesti ADHD:n kanssa 20–70 %:lla lapsista ja 35–50 %:lla
aikuisista «Michielsen M, Comijs HC, Semeijn EJ, ym. The comor...»333.
- Lapsuus- tai nuoruusiän ADHD suurentaa masennusriskiä, myös myöhemmin aikuisuudessa «Michielsen M, Comijs HC, Semeijn EJ, ym. The comor...»333, «Meinzer MC, Pettit JW, Viswesvaran C. The co-occur...»334, «Meinzer MC, Lewinsohn PM, Pettit JW, ym. Attention...»335, «Powell V, Agha SS, Jones RB, ym. ADHD in adults wi...»336, «Thapar A, Livingston LA, Eyre O, ym. Practitioner ...»337, «Riglin L, Leppert B, Dardani C, ym. ADHD and depre...»338.
- Osa masennuksen ja ADHD:n oireista, kuten keskittymisvaikeudet ja levottomuus, ovat
päällekkäisiä.
- ADHD:hen liittyvät oireet, kuten toiminnanohjauksen ongelmat ja mielialan vaihtelu, saatetaan tulkita depressioksi, ja ADHD:stä johtuva toimintakyvyn heikkeneminen voi aiheuttaa masennusoireita.
- Samanaikainen ADHD voi myös myötävaikuttaa siihen, ettei depressiosta toipuminen edisty tavanomaisesti.
- ADHD-oireiden psykososiaaliset hoitomuodot voidaan aloittaa osana masennuksen hoitoa
«Thapar A, Livingston LA, Eyre O, ym. Practitioner ...»337, «Remschmidt H, Global ADHD Working Group. Global co...»339, «Guo C, Assumpcao L, Hu Z. Efficacy of Non-pharmaco...»340.
- Lasten käyttäytymisen ohjaamiseen perustuvat hoidot (vanhemmuustaito-ohjaus) sekä tunne- ja sosiaalisten taitojen harjoittelu voivat lievittää myös masennusoireita.
- Kognitiivis-behavioraalinen terapia soveltuu sekä aikuisten ADHD:n että masennusoireiden hoitoon «ADHD-diagnoosin saaneilla aikuisilla kognitiivis-behavioraaliset interventiot vähentävät kliinisesti merkittävästi ADHD-oireita sekä samanaikaisia masennus- ja ahdistuneisuusoireita»A.
- Masennuksen lääkehoito toteutetaan Käypä hoito -suosituksen Depressio mukaisesti
«Depressio»13, «Depressio. Käypä hoito -suositus. Suomalaisen Lääk...»144.
- ADHD voi lisätä masennuslääkkeen aloitusvaiheeseen liittyvää itsetuhoisuuden riskiä «Ljung T, Chen Q, Lichtenstein P, ym. Common etiolo...»341.
- ADHD-lääkkeiden ja masennuksen yhteys on epäselvä.
- Kliinisen kokemuksen ja lääkkeiden myyntiluvissa ilmoitettujen tietojen perusteella stimulantit saattavat aiheuttaa haittavaikutuksena ärtyneisyyttä ja mielialaoireita.
- Meta-analyysien mukaan niillä ei kuitenkaan näytä olevan yhteyttä ahdistus- ja masennusoireisiin «Bryant A, Schlesinger H, Sideri A, ym. A meta-anal...»325, «Pozzi M, Carnovale C, Mazhar F, ym. Adverse Drug R...»342.
- Metyylifenidaattilääkityksellä on havaittu olevan myös masennusta ehkäisevää vaikutusta «Lee MJ, Yang KC, Shyu YC, ym. Attention-deficit hy...»343, «Krinzinger H, Hall CL, Groom MJ, ym. Neurological ...»344.
- Kaksisuuntaisessa mielialahäiriössä esiintyy masennus-, hypomania-, mania- tai sekamuotoisia sairausjaksoja ja vähäoireisia
tai oireettomia välivaiheita (ks. Käypä hoito -suositus Kaksisuuntainen mielialahäiriö
«Kaksisuuntainen mielialahäiriö»14, «Kaksisuuntainen mielialahäiriö. Käypä hoito -suosi...»145 sekä lisätietoa «ADHD ja kaksisuuntainen mielialahäiriö lapsuudessa ja nuoruudessa»41).
- Kaksisuuntaista mielialahäiriötä sairastavista aikuisista noin 10–20 %:lla, nuorista 30–50 %:lla ja lapsista 50–90 %:lla täyttyvät myös ADHD-diagnoosikriteerit «Wymbs BT, Canu WH, Sacchetti GM, ym. Adult ADHD an...»174, «Frías Á, Palma C, Farriols N. Comorbidity in pedia...»345, «Sadeghian Nadooshan MR, Shahrivar Z, Mahmoudi Ghar...»346, «Solberg BS, Halmøy A, Engeland A, ym. Gender diffe...»347, «Merikangas KR, Jin R, He JP, ym. Prevalence and co...»348, «Schiweck C, Arteaga-Henriquez G, Aichholzer M, ym....»349, «Miskowiak KW, Obel ZK, Guglielmo R, ym. Efficacy a...»350, «Pinna M, Visioli C, Rago CM, ym. Attention deficit...»351.
- ADHD-diagnoosin saaneista aikuisista noin 20 %:lla, nuorista 8–10 %:lla ja lapsista
mahdollisesti noin 6 %:lla on myös samanaikainen kaksisuuntainen mielialahäiriö «Wymbs BT, Canu WH, Sacchetti GM, ym. Adult ADHD an...»174, «Merikangas KR, Jin R, He JP, ym. Prevalence and co...»348, «Schiweck C, Arteaga-Henriquez G, Aichholzer M, ym....»349, «Miskowiak KW, Obel ZK, Guglielmo R, ym. Efficacy a...»350, «Salvi V, Ribuoli E, Servasi M, ym. ADHD and Bipola...»352, «Stutzman DL, Dopheide JA. Practice Pearls for Stim...»353.
- Samanaikaisuus näyttää altistavan tiheämmille oirejaksoille, itsemurhayrityksille sekä ahdistuneisuushäiriöille «Sadeghian Nadooshan MR, Shahrivar Z, Mahmoudi Ghar...»346.
- Häiriöiden oireet ovat samankaltaisia ja osin päällekkäisiä, mikä vaikeuttaa diagnostiikkaa, ks. lisätietoa «Erotusdiagnostiikka ADHD:ssä (ADHD, depressio, kaksisuuntainen mielialahäiriö, ahdistuneisuushäiriö ja traumaperäinen stressihäiriö)»44. ADHD:llä ja kaksisuuntaisella mielialahäiriöllä saattaa olla yhteisiä geneettisiä ja neurobiologisia riskitekijöitä, myös muiden häiriöiden kanssa «van Hulzen KJE, Scholz CJ, Franke B, ym. Genetic O...»354, «Als TD, Kurki MI, Grove J, ym. Depression pathophy...»355, «Khoury E, Acquaviva E, Purper-Ouakil D, ym. Meta-a...»356, «Hosang GM, Lichtenstein P, Ronald A, ym. Associati...»357.
- Lapsuusiän ADHD-diagnoosi näyttää liittyvän varhaisempaan mielialahäiriön puhkeamiseen, mutta pitkäaikaistutkimuksissa se ei kuitenkaan näytä lisäävän kaksisuuntaiseen mielialahäiriöön sairastumisen kokonaisriskiä «Sadeghian Nadooshan MR, Shahrivar Z, Mahmoudi Ghar...»346, «Schiweck C, Arteaga-Henriquez G, Aichholzer M, ym....»349, «Miskowiak KW, Obel ZK, Guglielmo R, ym. Efficacy a...»350, «Goldstein BI, Birmaher B, Carlson GA, ym. The Inte...»358, «Arnold LE, Van Meter AR, Fristad MA, ym. Developme...»359.
- Kaksisuuntaisen mielialahäiriön hoidossa tavoitteena on tasata mielialojen vaihtelua
ja ehkäistä jaksojen uusiutumista (ks. Käypä hoito -suositus Kaksisuuntainen mielialahäiriö
«Kaksisuuntainen mielialahäiriö»14, «Kaksisuuntainen mielialahäiriö. Käypä hoito -suosi...»145). Samanaikaisen ADHD:n tunnistaminen ja oireiden asianmukainen hoito tukee mielialahäiriön
hoitotavoitteiden saavuttamista.
- Lasten ja nuorten kaksisuuntaisen mielialahäiriön ja ADHD:n hoidossa keskeisiä ovat psykososiaaliset hoitomuodot «Connors MH. Paediatric bipolar disorder and its co...»360, «Brickman HM, Fristad MA. Psychosocial Treatments f...»361, «Stutzman DL, Dopheide JA. Practice Pearls for Stim...»353.
- Stimulantit voivat aiheuttaa harvinaisena haittavaikutuksena maniaoireita. Jos ADHD:n lääkehoidon aikana ilmenee äkillisiä maniaoireita, on lääkehoito keskeytettävä ja diagnostista arviota tarkennettava «https://fimea.fi/laakehaut_ja_luettelot/laakehaku»13.
- Stimulanttihoidon on epäilty aikaistavan manian puhkeamista «DelBello MP, Soutullo CA, Hendricks W, ym. Prior s...»362, «Jerrell JM, McIntyre RS, Park YM. Correlates of in...»363. Uudemmissa tutkimuksissa sen on kuitenkin havaittu samanaikaisten ADHD-oireiden hoidon yhteydessä vähentävän mielialaoireiden esiintymistä «Viktorin A, Rydén E, Thase ME, ym. The Risk of Tre...»364, «Tillman R, Geller B. Controlled study of switching...»365, «Chiorean A, Jones BDM, Murong M, ym. Prescribed ps...»366, «O'Connor H, Hutt Vater C, DiSalvo M, ym. Stimulant...»367, «Wang LJ, Shyu YC, Yuan SS, ym. Attention-deficit h...»368, «Jefsen OH, Østergaard SD, Rohde C. Risk of Mania A...»369.
- Sekä stimulanttien että atomoksetiinin käyttöä mielialaa tasaavan tai psykoosilääkityksen aikana pidetään turvallisena, jos se ADHD-oireiden hoidon vuoksi katsotaan välttämättömäksi «Perugi G, Vannucchi G. The use of stimulants and a...»370, «Pataki C, Carlson GA. The comorbidity of ADHD and ...»371, «Scheffer RE, Kowatch RA, Carmody T, ym. Randomized...»372, «Hah M, Chang K. Atomoxetine for the treatment of a...»373, «Findling RL, Short EJ, McNamara NK, ym. Methylphen...»374, «Chang K, Nayar D, Howe M, ym. Atomoxetine as an ad...»375, «Viktorin A, Rydén E, Thase ME, ym. The Risk of Tre...»364, «Miskowiak KW, Obel ZK, Guglielmo R, ym. Efficacy a...»350, «Pouchon A, Nasserdine R, Dondé C, ym. A systematic...»376, «McIntyre RS, Alsuwaidan M, Soczynska JK, ym. The e...»377.
- Huolellinen lääkehoidon suunnittelu ja tarkka oireseuranta lääkehoidon aloittamisen jälkeen voivat parantaa samanaikaista kaksisuuntaista mielialahäiriötä ja ADHD:tä sairastavan toimintakykyä «Viktorin A, Rydén E, Thase ME, ym. The Risk of Tre...»364.
- Psykoottiset häiriöt (ks. lisätietoa «ADHD ja psykoottiset oireet lapsilla ja nuorilla»43sekä Käypä hoito -suositus Skitsofrenia «Skitsofrenia»19, «Skitsofrenia. Käypä hoito -suositus. Suomalaisen L...»150) ovat harvinaisia lapsuudessa, mutta sairastumisriski suurenee nuoruudessa ja varhaisaikuisuudessa.
- Lapsuudessa tai nuoruudessa ADHD-diagnoosin saaneilla on suurentunut riski sairastua
psykoottiseen häiriöön «Dalsgaard S, Mortensen PB, Frydenberg M, ym. Assoc...»378, «Nourredine M, Gering A, Fourneret P, ym. Associati...»379.
- Psykoosin ennakko-oireet voivat muistuttaa ADHD:tä, eikä luotettava erotusdiagnostinen arvio ole aina etenkään lapsilla mahdollinen «Toba-Oluboka T, Dempster K. A Narrative Review Exp...»380.
- Psykoosiin sairastuneet näyttävät saavan ADHD-diagnoosin verrokkeja myöhemmin «Hollis C, Chen Q, Chang Z, ym. Methylphenidate and...»381.
- ADHD:hen liittyy suurentunut päihteiden käytön riski. Päihteiden käyttö (erityisesti kannabiksen käyttö) lisää psykoosiin sairastumisen riskiä «Toba-Oluboka T, Dempster K. A Narrative Review Exp...»380.
- Tutkimustieto ADHD-lääkkeiden vaikutuksesta psykoosiriskiin on jossain määrin ristiriitaista.
- ADHD-lääkkeiden haittavaikutuksena voi ilmetä harhaoireita «Mosholder AD, Gelperin K, Hammad TA, ym. Hallucina...»382, «Ross RG. Psychotic and manic-like symptoms during ...»383. Jos ADHD:n lääkehoidon aikana ilmenee äkillisiä psykoosioireita, on lääkehoito keskeytettävä. Haittavaikutuksena ilmenevät psykoosioireet yleensä lievittyvät nopeasti lääkkeen lopettamisen jälkeen «Toba-Oluboka T, Dempster K. A Narrative Review Exp...»380.
- Lääkehoidolla on havaittu olevan yhteys suurentuneeseen psykoosiriskiin «Björkenstam E, Pierce M, Björkenstam C, ym. Attent...»384, «Shyu YC, Yuan SS, Lee SY, ym. Attention-deficit/hy...»385. Riski saattaa olla suurempi amfetamiinilääkkeitä käytettäessä kuin metyylifenidaattia käytettäessä «Moran LV, Skinner JP, Shinn AK, ym. Risk of Incide...»386. Myös suuremmat lääkeannokset näyttävät liittyvän suurentuneeseen riskiin «Bieś R, Fojcik J, Warchala A, ym. The Risk of Meth...»387.
- Metyylifenidaattilääkitys ei kuitenkaan suurentanut 6–19-vuotiaiden psykoosiriskiä yli 20 000 potilaan ryhmässä 13 vuoden seuranta-aikana. Sen sijaan psykoosiriski näytti olevan hieman suurentunut ennen ADHD-lääkkeen aloitusta «Man KK, Coghill D, Chan EW, ym. Methylphenidate an...»388.
- Ruotsalaisessa rekisteriseurantatutkimuksessa psykoosiin sairastumisen riski ei näyttänyt suurenevan lääkkeen aloituksen jälkeen tai käytön aikana. Aiempi psykoosisairaus ei näyttänyt suurentavan psykoosiriskiä «Hollis C, Chen Q, Chang Z, ym. Methylphenidate and...»381.
- ADHD:tä voidaan hoitaa, vaikka henkilöllä olisi tai olisi aiemmin ollut psykoottinen
häiriö.
- ADHD:n psykososiaalisista hoitomuodoista voi olla hyötyä molempien häiriöiden oireiden hallinnassa «Toba-Oluboka T, Dempster K. A Narrative Review Exp...»380.
- ADHD:n lääkehoidossa samanaikaisen psykoosisairauden yhteydessä on noudatettava varovaisuutta. ADHD:n lääkehoitoa on mahdollista kokeilla vakiintuneen psykoosilääkityksen aikana pienillä aloitusannoksilla ja suurentamalla annosta vähitellen, mutta tutkimustietoa aiheesta on hyvin niukasti. Kliinisen kokemuksen perusteella pitkävaikutteiset valmisteet vaikuttavat olevan paremmin siedettyjä kuin nopeita pitoisuusvaihteluita aiheuttavat valmisteet. Hyvä sitoutuminen psykoosin (lääke)hoitoon lisää ADHD:n lääkehoidon turvallisuutta.
- Lapsuudessa tai nuoruudessa ADHD-diagnoosin saaneilla on suurentunut riski sairastua
psykoottiseen häiriöön «Dalsgaard S, Mortensen PB, Frydenberg M, ym. Assoc...»378, «Nourredine M, Gering A, Fourneret P, ym. Associati...»379.
ADHD:n arviointi ja hoito samanaikaisen päihdehäiriön yhteydessä
- Päihdehäiriöt ovat ADHD-diagnoosin saaneilla aikuisilla 2–3 kertaa yleisempiä kuin muulla väestöllä «Wymbs BT, Canu WH, Sacchetti GM, ym. Adult ADHD an...»174. Aikuisista, joilla on päihdehäiriö, arviolta vähintään joka viidennellä on myös ADHD «Young S, Abbasian C, Al-Attar Z, ym. Identificatio...»389, «Rohner H, Gaspar N, Philipsen A, ym. Prevalence of...»390.
- ADHD-lääkitys lapsuuden tai nuoruuden aikana ei suurenna eikä pienennä päihdehäiriön kehittymisen riskiä «Molina BSG, Kennedy TM, Howard AL, ym. Association...»391.
- ADHD-oireita ja hoidon tarvetta tulee systemaattisesti kartoittaa päihdehoidon yhteydessä.
ADHD-arviota tehdessä ja myös ADHD-hoidon aikana tulee toistuvasti arvioida potilaan
päihteiden käyttöä «Crunelle CL, van den Brink W, Moggi F, ym. Interna...»392, «Young S, Abbasian C, Al-Attar Z, ym. Identificatio...»389.
- ADHD-seulonnan ja diagnostiseen arviointiprosessiin liittyvien taustatietojen kartoittamisen
asiakirjatilauksineen voi aloittaa riippumatta siitä, käyttääkö henkilö ajankohtaisesti
päihteitä.
- Ks. video Päihdehäiriö ei saa estää ADHD:n tutkimista «Päihdehäiriö ei saa estää ADHD:n tutkimista (video)»6.
- Elämänkaarianamneesia tehdessä tulee huomioida ADHD-oireiden esiintyminen päihteettömien jaksojen aikana.
- Ennen ajankohtaisten ADHD-oireiden arviointia kannattaa pyrkiä yhden kuukauden päihteettömyyteen, mutta päihteettömyys ei kuitenkaan ole ehdoton vaatimus. Ajankohtaisten oireiden arviointia ei voi tehdä, jos henkilö on päihtynyt tai vieroitusoireinen. Vieroitusoireet voivat joskus muistuttaa ADHD-oireita.
- ADHD-potilailla, joilla on myös päihdehäiriö, on tyypillisesti useita muita samanaikaisia psykiatrisia häiriöitä, joita tulisi kartoittaa strukturoituja diagnostisia haastattelumenetelmiä käyttäen.
- ADHD-seulonnan ja diagnostiseen arviointiprosessiin liittyvien taustatietojen kartoittamisen
asiakirjatilauksineen voi aloittaa riippumatta siitä, käyttääkö henkilö ajankohtaisesti
päihteitä.
- Suositus 23: ADHD:n ja päihdehäiriön hoito on pyrittävä toteuttamaan samanaikaisesti
huomioiden häiriöiden vaikutus toisiinsa.
- Samanaikaisessa hoidossa toteutetaan molempien häiriöiden hoitosuosituksia sekä psykososiaalisen että lääkkeellisen hoidon suhteen. Hoitovastetta seurataan molempien häiriöiden suhteen. Myös mahdolliset muut häiriöt hoidetaan samaan aikaan.
- Ks. video ADHD:ta voidaan hoitaa samaan aikaan päihdehäiriön kanssa «ADHD:ta voidaan hoitaa samaan aikaan päihdehäiriön kanssa (video)»7.
- Suositus 24: Kun ADHD ja päihdehäiriö esiintyvät samanaikaisesti, tulee ADHD-oireiden
diagnostinen arviointi ja hoidon aloitus toteuttaa hoitoyksiköissä, joissa on osaamista
sekä päihdehäiriöiden että ADHD:n arvioinnista ja hoidosta.
- Hoidon tulee sisältää sekä psykososiaalisia hoitomenetelmiä, kuten samanaikaisesti ADHD:n ja päihdehäiriön hoitoon suunnattua kognitiivis-behavioraalista terapiaa, että lääkehoitoa «Crunelle CL, van den Brink W, Moggi F, ym. Interna...»392. Kelan kuntoutuspsykoterapiaa harkittaessa tulee huomioida Kelan vaatimus riittävästä päihteettömyydestä.
- Jos henkilöllä on samanaikaisesti sekä vaikea-asteinen päihdehäiriö että muuta runsasta psykiatrista samanaikaissairastavuutta, hoito vaatii tiivistä seurantaa.
- Koska aktiivinen päihteidenkäyttö vaikuttaa ADHD:n hoitoon, on suositeltavaa, että hoidossa tähdätään päihteidenkäytön lopettamiseen tai vähäiseen päihteidenkäyttöön eli käyttöön, josta ei koidu hoidettavalle haittaa.
- Lääkehoidon tarvetta ja hyötyä tulee arvioida tapauskohtaisesti ja usein eri mittarein,
eikä lääkehoidon toteutuksen osalta voida edellyttää täysraittiutta.
- Ennen ADHD:n lääkehoidon aloittamista olisi suotavaa, ettei henkilö käytä päihteitä säännöllisesti, esimerkiksi useammin kuin kerran viikossa. Päihteidenkäyttö ja siihen liittyvät riskit tulee arvioida yksilöllisesti eri päihteiden osalta, eikä ehdottomia aikarajoja tai käyttömääriä voida asettaa.
- ADHD:n lääkehoito psykostimulanteilla vähentää todennäköisesti ADHD-oireita henkilöillä,
joilla on ADHD ja samanaikainen päihdehäiriö «ADHD:n lääkehoito psykostimulanteilla todennäköisesti vähentää ADHD-oireita henkilöillä, joilla on ADHD ja samanaikainen päihdehäiriö.»B.
- Tavanomaisesti käytettyjä suuremmat psykostimulanttiannokset näyttävät yhdistyvän parempaan hoitovasteeseen henkilöillä, joilla on ADHD:n lisäksi päihdehäiriö «Carpentier PJ, Levin FR. Pharmacological Treatment...»395, «Crunelle CL, van den Brink W, Moggi F, ym. Interna...»392.
- Atomoksetiini saattaa vähentää ADHD-oireita henkilöillä, joilla on samanaikainen ADHD ja alkoholihäiriö (ks. Käypä hoito -suositus Alkoholiongelmat, näytönastekatsaus «Alkoholiongelmaisella ADHD-potilaalla atomoksetiinista saattaa olla hyötyä ADHD:n oireiden vähentämiseen, mutta sillä ei ole vaikutusta alkoholinkäyttöön.»C).
- ADHD:n lääkehoito ilmeisesti vähentää vähän tai kohtuullisesti päihteidenkäyttöä ainakin
lyhytaikaisesti henkilöillä, joilla on samanaikaisesti sekä ADHD että päihdehäiriö
«ADHD:n lääkehoito ilmeisesti vähentää vähän tai kohtuullisesti päihdekäyttöä ainakin lyhytaikaisesti henkilöillä, joilla on samanaikaisesti sekä ADHD että päihdehäiriö.»B.
- Nuorten samanaikaisen päihdehäiriön ja ADHD:n hoidosta on huomattavan vähän tutkimusta. Vähäistä näyttöä on siitä, että pitkävaikutteiset stimulantit ja ei-stimulantit olisivat hyödyllisiä myös nuorilla, joilla on samanaikainen päihdehäiriö «Zaso MJ, Park A, Antshel KM. Treatments for Adoles...»396.
- Myös nikotiini on päihde, ja henkilöiden, joilla on ADHD, on todettu tupakoivan muita useammin «van Amsterdam J, van der Velde B, Schulte M, ym. C...»393. Stimulanttihoidon on todettu vähentävän tupakointia «Schoenfelder EN, Faraone SV, Kollins SH. Stimulant...»394.
Ennuste ja seurannaisvaikutukset
Terveysriskit
- ADHD-oireisiin liittyy tapaturma-alttiutta ja suurentunut riski joutua vaaratilanteisiin
(ks. lisätietoa «ADHD ja tapaturmariski»77), «Lee LC, Harrington RA, Chang JJ, ym. Increased ris...»397, «Palili A, Kolaitis G, Vassi I, ym. Inattention, hy...»398, «Garzon DL, Huang H, Todd RD. Do attention deficit/...»399, «Erskine HE, Norman RE, Ferrari AJ, ym. Long-Term O...»400, «Libutzki B, Neukirch B, Kittel-Schneider S, ym. Ri...»401. Samanaikaisella käytöshäiriöllä tai päihdehäiriöllä ja lasten ja nuorten puutteellisella
valvonnalla voi myös olla merkitystä «Schwebel DC, Speltz ML, Jones K, ym. Unintentional...»402, «Schwebel DC, Hodgens JB, Sterling S. How mothers p...»403, «So M, Dziuban EJ, Pedati CS, ym. Childhood Physica...»404
- Impulsiivisuus ilmenee tapaturma-alttiutena myös nuoruus- ja aikuisiässä, jolloin se näkyy erityisesti liikenteessä sääntörikkomuksina ja suurentuneena onnettomuusalttiutena «Fischer M, Barkley RA, Smallish L, ym. Hyperactive...»405.
- ADHD:n lääkehoito näyttää pienentävän onnettomuusriskiä kaikissa ikäryhmissä «Brunkhorst-Kanaan N, Libutzki B, Reif A, ym. ADHD ...»406, «Ruiz-Goikoetxea M, Cortese S, Aznarez-Sanado M, ym...»407, «Vasiliadis HM, Lunghi C, Rahme E, ym. ADHD medicat...»408.
- ADHD:hen on joissakin tutkimuksissa liitetty suurentunut dementiasairauden riski, mutta tutkimustieto on ristiriitaista, myös etiologisista yhteyksistä «Carr RH, Eom GD, Brown EE. Attention-Deficit/Hyper...»409, «Becker S, Chowdhury M, Tavilsup P, ym. Risk of neu...»410.
Vaikutus toimintakykyyn ja suoriutumiseen
- Lapsuus- tai nuoruusiän ADHD on yhteydessä tavallista heikompaan suoriutumiseen opinnoissa
ja työelämässä «Tervo T, Michelsson K, Launes J, ym. A Prospective...»250, «Erskine HE, Norman RE, Ferrari AJ, ym. Long-Term O...»400, «Stein DS, Blum NJ, Barbaresi WJ. Developmental and...»411, «Mordre M, Groholt B, Sandstad B, ym. The impact of...»412.
- Pitkittäistutkimusten alkuvaiheissa ADHD:n hoito ja kuntoutus ovat olleet erilaisia kuin nykyisin, mikä voi heikentää tutkimustulosten yleistettävyyttä nykyaikaan.
- ADHD:n vaikutusta nuoren opiskelusuuntauksen valintaan ja työllistymisen edellytyksiin
on arvioitava yksilöllisesti, ks. lisätietoa ADHD-oireisten opiskelijoiden vahvuusperustainen
opinto- ja uraohjaus «ADHD-oireisten opiskelijoiden vahvuusperustainen opinto- ja uraohjaus»78. Arvioinnissa on huomioitava ADHD:n vaikeusaste, kognitiivinen ja muu kyvykkyys sekä
samanaikaissairastavuus.
- ADHD-diagnoosi voi estää toimimisen sellaisissa ammateissa, joihin liittyy terveydellisiä vaatimuksia.
- ADHD:hen liitetään positiivisia ominaisuuksia, kuten luovuus, energisyys ja riskinottokyky, jotka voivat tukea työelämässä menestymistä «Nordby ES, Guribye F, Nordgreen T, ym. Silver lini...»413, «Huang W, Yuan C, Li M. Person-Job Fit and Innovati...»414, «Vaaramo M. Studies on occupational choice, tempera...»415.
- Samanaikaiset oppimisvaikeudet vaikuttavat opinnoissa suoriutumiseen «Seidman LJ, Biederman J, Weber W, ym. Neuropsychol...»416.
- ADHD on huomioitava ajoterveyttä arvioitaessa «https://www.traficom.fi/fi/saadokset/ajoterveyden-arviointiohjeet-terveydenhuollon-ammattilaisille»15 (ks. myös lisätietoa «ADHD ja autoilu»79).
- ADHD-diagnoosi estää liikenneturvallisuustehtävissä toimimisen (esim. liikennelentäjän ja raidekuljettajan tehtävät).
- Ajoterveysvaatimukset eivät täyty, jos häiriöön liittyy vaikea-asteinen tarkkaavaisuuden heikentyminen, voimakas elämyshakuisuus tai impulsiivisuus.
- Erityisesti impulsiivisuus ja aggressiivisuus ovat merkittäviä riskitekijöitä liikenteessä. Asianmukainen lääkehoito yleensä parantaa ajokykyä «Chang Z, Lichtenstein P, D'Onofrio BM, ym. Serious...»417.
- Nuori, jolla on ADHD-diagnoosista huolimatta hyvä toimintakyky ilman lääkehoitoa eikä
merkittäviä samanaikaishäiriöitä, voi soveltua asepalvelukseen «Halt AH, Uusitalo J, Niemi P, ym. Military perform...»418, ks. lisätietoa «ADHD ja asepalvelus»80
- Arvio tulee tehdä yksilökohtaisesti (Terveystarkastusohje «https://puolustusvoimat.fi/documents/1948673/2015558/Terveystarkastusohje/95c74723-da6f-47f8-b1cf-964fc3affb73/Terveystarkastusohje.pdf»16).
Vaikutus rikollisuuteen
- Henkilöillä, joilla on ADHD, on lisääntynyt riski syyllistyä rikoksiin tai joutua
rikosten uhreiksi «Faraone SV, Banaschewski T, Coghill D, ym. The Wor...»11. Ks. lisätietoa «ADHD:n yhteys rikollisuuteen»81.
- Meta-analyysit ja systemaattiset katsaukset ovat osoittaneet, että ADHD on muuta väestöä yleisempää vankien keskuudessa. Arviot ADHD:n esiintyvyydestä vankien joukossa vaihtelevat 9 %:n ja 45 %:n välillä.
- Vuonna 2023 julkaistussa suomalaisessa vankitutkimuksessa tunnistettiin ADHD-oirekuva 46 %:lla miehistä ja 43 %:lla naisista «Rautanen M, Harald K, Tyni S. Vankien terveys ja h...»419. He olivat nuorempia, harvemmin ensikertalaisia ja vähemmän kouluttautuneita muihin vankeihin verrattuna. ADHD-oireiset päätyivät kurinpidolliseen eristykseen muita useammin, mikä voi viitata vaikeuteen sopeutua vankilaympäristöön.
- ADHD-lääkitys näyttäisi olevan yhteydessä vähäisempään rikolliseen toimintaan ja parempaan toimintakykyyn. Ks. tarkemmin lisätietoa «ADHD:n yhteys rikollisuuteen»81.
- Suositus 25: Työryhmä suosittelee ADHD:n seulomista, arvioimista ja hoitamista vankiterveydenhuollossa
paitsi yksilöllisen hyvinvoinnin vuoksi, myös laitosturvallisuuden parantamiseksi
ja uusintarikollisuuden vähentämiseksi «AADPA. Australian Evidence-Based Clinical Practice...»124, «Kriminalvården. 2021. Neuropsykiatrisk utredningsr...»420.
- Vankiterveydenhuollossa ADHD:tä tulee arvioida ja hoitaa muuta terveydenhuoltoa aktiivisemmin, koska kyseessä on suuren perusesiintyvyyden väestö.
Vaikutus kuolleisuuteen
- Systemaattisessa meta-analyysissä ADHD-diagnoosin saaneiden kokonaiskuolleisuus oli
suurempi kuin verrokkiväestön. Kuolleisuuden lisääntyminen liittyy ei-luonnollisiin
kuolemiin, kuten myrkytyksiin, tapaturmiin ja itsemurhiin. Luonnollisista syistä johtuva
kuolleisuus ei ollut tilastollisesti suurempi «Catalá-López F, Hutton B, Page MJ, ym. Mortality i...»421.
- Ruotsalaisessa rekisteritutkimuksessa psykiatriset samanaikaishäiriöt ja päihdehäiriö lisäsivät ADHD-diagnoosin saaneiden kuolleisuutta «Sun S, Kuja-Halkola R, Faraone SV, ym. Association...»422.
- ADHD:n lääkehoito näyttää väestötason rekisteritutkimuksissa vähentävän erityisesti tapaturmiin liittyvää kuolleisuutta «Vasiliadis HM, Lunghi C, Rahme E, ym. ADHD medicat...»408, «Li L, Zhu N, Zhang L, ym. ADHD Pharmacotherapy and...»423.
Vaikutus elämänlaatuun
- ADHD heikentää lasten elämänlaatua sukupuolesta tai ADHD:n alatyypistä riippumatta. Elämänlaatu heikkenee suunnilleen yhtä paljon kuin fyysisissä kroonisissa sairauksissakin, mutta lähinnä psykososiaalisella osa-alueella «Danckaerts M, Sonuga-Barke EJ, Banaschewski T, ym....»424.
- ADHD heikentää myös aikuisten elämänlaatua «Faraone SV, Banaschewski T, Coghill D, ym. The Wor...»11. ADHD:n aiheuttama haitta voi painottua myös esimerkiksi akateemiseen suoriutumiseen tai työelämässä toimimiseen.
- ADHD:n aktiivinen hoito näyttää vähentävän kielteisiä seurannaisvaikutuksia ja terveysriskejä «Mohr-Jensen C, Steinhausen HC. A meta-analysis and...»425, «Connor DF, Carlson GA, Chang KD, ym. Juvenile mala...»426 sekä parantavan elämänlaatua ja toimintakykyä «Prasad S, Harpin V, Poole L, ym. A multi-centre, r...»427.
Työryhmän suositus hoidon porrastuksesta
- Suositus 26: Työryhmä suosittaa, että jokaisella hyvinvointialueella on selkeä ohjeisto
levottomuuden ja tarkkaamattomuuden selvittämiseksi ja paikallisen ADHD-hoitoketjun
kuvaus.
- Hoitoketjussa sovitetaan eri toimijoiden osuudet yhteen niin, että esimerkiksi diagnosointi on yhtenäistä, hoidon eri osa-alueet mahdollistuvat ja konsultaatiotoiminta on sujuvaa.
- Perusterveydenhuollon ja erikoissairaanhoidon välisestä työnjaosta ja yhteistyöstä sovittaessa otetaan huomioon paikalliset osaajaresurssit ja työnjako, mutta hoitoon pääsyn on oltava tasa-arvioista.
- Hoitoketjussa kuvataan myös varhaiskasvatuksessa, sivistystoimessa ja muissa oppilaitoksissa toteutettavat tukitoimet ja interventiot sekä yhteistyö eri toimijoiden kesken.
- Hoitoketjukuvauksessa määritellään, miten
- psykologiset ja muut mahdollisesti tarvittavat erityistutkimukset järjestetään
- psykososiaaliset hoidot (kuten vanhemmuustaito-ohjelmat) toteutetaan
- erikoissairaanhoidon tai vaativien palvelujen konsultaatiotuki järjestetään
- hoidon jatkuvuus varmistetaan eri tahojen välillä ja eri kehitysvaiheissa, esimerkiksi aikuistuvan nuoren hoidon siirtyessä opiskeluterveydenhuollon, työterveyshuollon tai terveysaseman välillä.
- Suositus 27: Työryhmä suosittaa, että ADHD:n diagnostiikka ja hoidon seuranta keskitetään myös perustason palveluissa neurokehityksellisiin oireyhtymiin ja niiden erotusdiagnostiikkaan perehtyneille työntekijöille.
- Tärkeänä pidetään sitä, että
- perustason palveluissa, esimerkiksi oppilashuollossa ja lasten ja nuorten mielenterveyspalveluissa, on käytettävissä riittävä määrä työntekijöitä, joiden työnkuvaan kuuluvat ADHD:n potilas- ja omaisneuvonta, arjen sujuvuutta tukevien menetelmien sekä varhaiskasvatuksen, koulun ja oppilaitosten tukitoimien ohjaus ja esimerkiksi strukturoitu vanhempainohjaus
- oppilashuollossa on alueelliset resurssit huomioiden sovittu eri ammattilaisten rooleista ja yhteistyöstä sekä alkukartoituksessa että tukitoimien toteutuksessa
- työterveyshuolto osallistuu ADHD-oireista johtuvien työssä ilmenevien vaikeuksien ratkaisemiseen
- vankiterveydenhuollossa on otettu huomioon ADHD:n hoito
- ADHD-diagnoosin tekevällä ja mahdollisen lääkityksen aloittavalla lääkärillä on mahdollisuus konsultoida erikoislääkäriä
- erikoissairaanhoito järjestää riittävästi diagnosoinnin ja hoidon onnistumista tukevia joustavia konsultaatiomahdollisuuksia ja koulutusta
- ADHD-diagnoosin saaneen ja hänen perheensä on mahdollista osallistua alueellaan järjestettäviin ensitietopäiviin, ryhmämuotoisiin kuntoutuksiin ja tukiryhmiin riippumatta siitä, missä hoitovastuu on
- useamman perheenjäsenen ADHD:n hoito ja kuntoutus toteutetaan koordinoidusti.
- Lasten ja nuorten alkuarvio, ADHD:n diagnostiikka ja hoidon toteutus
- Kun huoli lapsen tai nuoren keskittymättömyydestä ja ylivilkkaudesta herää, perheen
tukeminen sekä tilanteen mukaiset varhaiskasvatuksen tai koulun tukitoimet aloitetaan
heti, jo ennen tarkempaa diagnostista arviota. Ensisijainen vastuu lapsen tai nuoren
varhaisen tuen suunnittelemisesta ja järjestämisestä on alueen peruspalveluilla (kasvatus-
ja perheneuvonta, perusterveydenhuolto, varhaiskasvatus, koulu tai muu vastaava taho
yhteistyössä perheen kanssa).
- Jos tukitoimet lievittävät ongelmia, tarkempaa arviota ei välttämättä tarvita.
- Jos lapsen tai nuoren ongelmat jatkuvat tukitoimista huolimatta, hänet ohjataan perusterveydenhuollon lääkärin arvioitavaksi tai tarpeelliseksi arvioituihin muihin tutkimuksiin esimerkiksi lasten ja nuorten perustason mielenterveyspalveluihin (LANU). Tukitoimien jatkuminen tutkimusten aikanakin on varmistettava.
- Tarkempaa ADHD-oireiden diagnostista arviota tarvitaan, mikäli toteutuneista tukitoimista huolimatta esiintyy pitkäaikaisesti toimintakykyä ja arkea haittaavaa impulsiivisuutta, aktiivisuuden ja tarkkaavuuden säätelyn vaikeuksia ja harkitaan diagnoosia vaativaa kuntoutusta tai lääkehoitoa.
- Hoitoketjussa on otettava huomioon, että vaikeaoireisten lasten ja nuorten pitäisi saada diagnostiset tutkimukset ja riittävän intensiivistä hoitoa mahdollisimman nopeasti ilman pitkää jonottamista.
- Lasten ja nuorten diagnostinen arvio ja hoito- ja kuntoutussuunnitelma tehdään moniammatillisesti
ensisijaisesti perusterveydenhuollon palveluissa, ellei erityistä perustetta vaativampiin
palveluihin ole esimerkiksi erotusdiagnostisista syistä.
- Mahdollisesti lääkekokeilua tarvitsevat alle 6-vuotiaat lapset ohjataan erikoissairaanhoitoon.
- Tarvittavien tietojen (ks. kohta Diagnosointi «A3»4 sekä lisätietoa «ADHD-oireiden diagnostista arviointia varten koottavia tietoja»26 ja «ADHD:n diagnostisen arvion muistilista»28) kokoaminen esimerkiksi neuvolan ja kouluterveydenhuollon kirjauksista tehdään perustason palveluissa.
- Moniammatillista työtä voidaan toteuttaa ryhmässä, johon osallistuvat lapsen ja nuoren
sekä hänen huoltajansa lisäksi esimerkiksi kouluterveydenhoitaja (elintapojen kartoitus
ja tuki), ADHD:n diagnostiikkaan ja hoitoon perehtynyt lääkäri, psykologi sekä varhaiskasvatuksen
ja koulun tukitoimiin, psykoedukaatioon ja perheiden tukemiseen perehtyneitä työntekijöitä,
jotka huolehtivat suunnitelman toteuttamisesta.
- Hoitovasteen ja kuntoutussuunnitelman tavoitteiden toteutumisen seuranta-aikataulusta ja vastuutahosta sovitaan kuntoutussuunnitelmassa.
- Kun huoli lapsen tai nuoren keskittymättömyydestä ja ylivilkkaudesta herää, perheen
tukeminen sekä tilanteen mukaiset varhaiskasvatuksen tai koulun tukitoimet aloitetaan
heti, jo ennen tarkempaa diagnostista arviota. Ensisijainen vastuu lapsen tai nuoren
varhaisen tuen suunnittelemisesta ja järjestämisestä on alueen peruspalveluilla (kasvatus-
ja perheneuvonta, perusterveydenhuolto, varhaiskasvatus, koulu tai muu vastaava taho
yhteistyössä perheen kanssa).
- Aikuisten ADHD:n tutkimusten ja hoidon toteutus
- Ellei aikuiselle aiemmin ole tehty ADHD-diagnoosia, diagnostisen arvion tekee ensisijaisesti psykiatrian alojen erikoislääkäri tai toissijaisesti muu neurokehityksellisiin oireyhtymiin ja psykiatrisiin häiriöihin perehtynyt lääkäri konsultoiden tarvittaessa psykiatrian alojen erikoislääkäriä.
- Psykiatrian alojen erikoislääkärin konsultaatio on välttämätön, jos ensimmäisen ADHD:n lääkehoidon aloittava lääkäri ei ole erikoislääkäri. Jatkohoito voidaan vakiintuneessa vaiheessa toteuttaa siten, että lääkityksen jatkossa määräävä lääkäri konsultoi tarvittaessa ADHD:n hoitoon perehtynyttä lääkäriä.
- Julkisen sektorin palveluissa aloitetun hoidon seuranta on diagnoosin tehneen tahon mukaisesti opiskeluterveydenhuollon, perusterveydenhuollon tai työterveyshuollon lääkärin ja hänen työparinsa vastuulla, ellei hoitoketjukuvauksessa ole toisin sovittu.
- Erikoissairaanhoidon vastuulla ovat erikoissairaanhoitoa tarvitsevien potilaiden erotusdiagnostiset selvittelyt ja
niihin kuuluvat lisätutkimukset, vaativien lääkehoitojen aloittaminen, vaativan hoidon
ja kuntoutuksen suunnittelu sekä jatkohoidosta ja -seurannasta sopiminen. Lisäksi
erikoissairaanhoidon tehtäviin kuuluvat riittävien konsultaatiomahdollisuuksien ja
koulutuksen järjestäminen.
- Erikoissairaanhoidon arviota tarvitaan, jos
- perusterveydenhuollon hoito- ja kuntoutustoimet ovat osoittautuneet konsultaatiotuesta huolimatta riittämättömiksi
- tarvitaan erityistä osaamista vaativaa erotusdiagnostista arviointia
- lääkehoidon toteutuksessa tai hoitovasteessa on ongelmia, jotka eivät ratkea konsultaatiotuen avulla tai
- kokonaistilanteen ongelmallisuuden vuoksi tarvitaan erikoissairaanhoidon osaamista tai usean erikoisalan yhteistyötä.
- Erikoissairaanhoidon arviota tarvitaan, jos
- Erikoissairaanhoidon lähete ohjataan ikäryhmän mukaisesti
- avopediatrian poliklinikalle tai avopediatrian konsultaatioon, jos lapsen tai nuoren
oirekuvaan liittyy
- tarve somaattisten sairauksien huomioimiseen tai sulkemiseen pois
- vaikeuksia löytää sopivaa lääkehoitoa
- lastenpsykiatrialle, jos lapsen oirekuvaan liittyy
- merkittäviä tai vaikeutuvia psyykkisiä oireita, esimerkiksi vaikeita käytösongelmia tai vakavaa masennusta, tai
- lapsen ja vanhemman välisiä merkittäviä vuorovaikutusongelmia eivätkä ongelmat johdu pelkästään huolenpidon puutteista, kuten vanhemman päihteidenkäytöstä tai psyykkisestä sairaudesta
- nuorisopsykiatrialle, jos nuoren oirekuvaan liittyy
- merkittäviä tai vaikeutuvia psyykkisiä oireita
- vaikeita käyttäytymisen häiriöitä tai
- päihdeongelma
- lastenneurologialle tai neurologialle, jos
- epäillään neurologista sairautta (esim. neurofibromatoosi, epilepsia, muistisairaus) tai lapsella tai nuorella kehitysvammaisuutta
- aikuispsykiatrialle, jos
- muu psykiatrinen tai somaattinen sairaus tai päihdehäiriö vaikeuttaa ADHD:n lääkehoidon suunnittelua
- lääkehoidolle ei ole saatu riittävää hoitovastetta tai
- lääkehoidon haittavaikutukset ovat estäneet lääkkeen käytön.
- avopediatrian poliklinikalle tai avopediatrian konsultaatioon, jos lapsen tai nuoren
oirekuvaan liittyy
Suomalaisen Lääkäriseuran Duodecimin, Suomen Lastenneurologisen yhdistyksen, Suomen Nuorisopsykiatrisen Yhdistyksen ja Suomen Lastenpsykiatriyhdistyksen asettama työryhmä
ADHD (aktiivisuuden ja tarkkaavuuden häiriö) -suosituksen historiatiedot «ADHD (aktiivisuuden ja tarkkaavuuden häiriö), Käypä hoito -suosituksen historiatiedot»82
Puheenjohtaja ja kokoava kirjoittaja:
Anita Puustjärvi, lastenpsykiatrian erikoislääkäri, lastenpsykoterapian erityispätevyys, lastenpsykiatrian ylilääkäri, asiantuntijalääkäri; Pohjois-Savon hyvinvointialue, KYS ja Kela
Jäsenet:
Silja Kosola, LT, yleislääketieteen erikoislääkäri, nuorisolääketieteen dosentti, nuorisolääketieteen erityispätevyys; Länsi-Uudenmaan hyvinvointialue
Maria Laine, LL, lastenneurologian erikoislääkäri, apulaisylilääkäri; Tays, lastentautien vastuualue, lastenneurologian yksikkö
Sami Leppämäki, LT, psykiatrian erikoislääkäri, psykiatrian dosentti, psykoterapian erityispätevyys, erikoisalajohtaja; Terveystalo
Krista Nuotio, LT, neurologian erikoislääkäri, tutkija, HUS Neurokeskus, neurologia; Käypä hoito -toimittaja, Suomalainen Lääkäriseura Duodecim
Vesa Närhi, PsT, dosentti, yliopistotutkija; Jyväskylän yliopisto, kasvatustieteen laitos
Hertta Ollikainen, LL, lastentautien erikoislääkäri, lastenneuvola- ja kouluterveydenhuoltotyön erityispätevyys; Kymenlaakson hyvinvointialue
Leena Pihlakoski, LL, lastenpsykiatrian erikoislääkäri, psykoterapian erityispätevyys; LP Lastenpsykiatripalvelut
Hanna Putkonen, LT, psykiatrian ja oikeuspsykiatrian erikoislääkäri, oikeuspsykiatrian dosentti
Maria Sumia, LL, nuorisopsykiatrian erikoislääkäri, lastentautien erikoislääkäri; Pirkanmaan hyvinvointialue, Tays, nuorisopsykiatrian poliklinikka
Maarit Virta-Jämiä, PsT, kliinisen neuropsykologian dosentti, neuropsykologian erikoispsykologi, kouluttajapsykoterapeutti; Resolvo Oy
Asiantuntijat:
Anne-Mari Borg, LT, lastenpsykiatrian erikoislääkäri, apulaisylilääkäri; Pirkanmaan hyvinvointialue, lastenpsykiatrian osasto- ja akuuttihoidon yksikkö
Jyrki Huusko, KT, koulunkehittämistutkimuksen dosentti, johtava rehtori; Itä-Suomen yliopiston harjoittelukoulu
Tarja Kaipainen, TtM, laillistettu ravitsemusterapeutti, Pohjois-Savon hyvinvointialue; Käypä hoito -toimittaja (ravitsemustiede), Suomalainen Lääkäriseura Duodecim
Anu Kippola-Pääkkönen, YTT, toimintaterapeutti, erityisasiantuntija; Lapin ammattikorkeakoulu
Liisa Klenberg, PsT, neuropsykologian erikoispsykologi; Mehiläinen Terapiaklinikka Helsinki
Jorma Komulainen, LT, dosentti, lastentautien ja lastenendokrinologian erikoislääkäri; asiantuntijalääkäri, Suomalainen Lääkäriseura Duodecim
Solja Niemelä, LT, päihdelääketieteen ja psykiatrian professori; Turun yliopisto
Leea Oikarainen, lastenneurologian erikoislääkäri, perinnöllisyyslääketieteen erikoistuva lääkäri; Tays
Markku Partinen, LKT, neurologian dosentti, professori, unilääketieteen ja liikennelääketieteen erityispätevyys, vastuututkija, kliiniset neurotieteet; Clinicum, Helsingin yliopisto
Hanna Raaska, LT, lastenpsykiatrian erikoislääkäri, osastonylilääkäri; HUS Lastenpsykiatria
Outi Saarenpää-Heikkilä, LT, lastenneurologian dosentti, lastenneurologian ja lastentautien erikoislääkäri, unilääketieteen erityispätevyys, ylilääkäri; Tays, lastenklinikka
Arja Tuunainen, LT, biologisen psykiatrian dosentti, kliinisen neurofysiologian ja psykiatrian erikoislääkäri, psykoterapeutti
Tanja Äärelä, KT, erityispedagogiikan professori; Lapin yliopisto
Viiteryhmä:
Potilasviiteryhmän asiantuntijat eivät ole osallistuneet päätöksentekoon hoitosuosituksen sisällöstä ja muotoiluista.
Potilaiden osallisuus on toteutettu Käypä hoito -suosituksen ADHD (aktiivisuuden ja tarkkaavuuden häiriö) yhteydessä kahdella viiteryhmän Teams-kokouksella. Viiteryhmä on antanut suosituksesta myös lausunnon.
Jäsenet:
Larissa Nykänen, Jyväskylä
Heini Lehtonen, Äänekoski
Samuli Kaukonen, Ikaalinen
Pasi Helosvuori, Jyväskylä
Katariina Berggren, ADHD-liitto
Minni Metso, Helsinki
Sidonnaisuudet
Sidonnaisuusilmoitukset on kerätty 19.5.2025 julkaistun suosituksen laatimisen yhteydessä.
Silja Kosola: Koulutustoiminta: luentopalkkioita vuodesta 2023 lähtien: Duodecim, Edumar oy, Professio oy, Mehiläinen oy, Merck oy. Luottamustoimet terveydenhuollon alalla: Suomen nuorisolääkärit ry, hallituksen jäsen ja erityispätevyystoimikunnan sihteeri; WHO Europe and European Observatory on Health Systems and Policies, external advisor, European Public Health Association, Section for Child and Adolescent Public Health, member of steering committee; International Association for Adolescent Health, Euroopan kongressin järjestelytoimikunta.
Maria Laine: Sivutoimet: lastenneurologian koulutusvastaavalääkäri (KoVa-lääkäri), Tampereen yliopisto. Kongressit ja seminaarit: Novartis Gene Therapies. Toiminta terveydenhuollon ohjaukseen pyrkivissä hankkeissa: ADHD:n hoitoketju ja kielihäiriöisyyden hoitoketju, Pirha.
Sami Leppämäki: Sivutoimet: yksityislääkäri, Terveystalo, Helsinki; jäsen, sosiaaliturva-asioiden muutoksenhakulautakunta. Koulutustoiminta: Biocodex, Lundbeck, Takeda – luentopalkkio, Takeda – luento- ja asiantuntijapalkkio koulutusmateriaalin tuottamisesta. Kongressit ja seminaarit: Lundbeck, Takeda.
Krista Nuotio: Sivutoimet: yksityisvastaanotto, Terveystalo. Luottamustoimet terveydenhuollon alalla: Helsingin lääkäripäivien ohjelmatyöryhmän jäsen.
Vesa Närhi: Koulutustoiminta: kouluttaja Niilo Mäki -säätiö ja useat kunnat.
Hertta Ollikainen: Sivutoimet: lääkärinvastaanotto, Mehiläinen 3/2025– ja Pihlajalinna 4/2025–. Koulutustoiminta: luentopalkkio, Lääkäriliitto. Luottamustoimet terveydenhuollon alalla: Lastenlääkäriyhdistyksen Avopediatrit-jaoston hallituksen jäsen 2025–. Muut sidonnaisuudet: osakeomistus, Oma Partners, majoittuminen Tuohilammella seminaarin yhteydessä, Orion.
Leena Pihlakoski: Sivutoimet: vastaanotto yksityisenä ammatinharjoittajana, Terveystalo. Koulutustoiminta: luentopalkkiot: Hogrefe Oy, Biocodex Oy, Takeda Oy, Kirsi Consulting Oy, Suomen Lastenpsykiatriyhdistys, Suomen Lääkäripäivät, Tampereen Yliopisto, Turun Yliopisto, Oulun Yliopisto. Julkaisu/tekijänpalkkiot: PS-kustannus, Duodecim.
Hanna Putkonen: Sivutoimet: kansallisen valvontaviranomaisen asiantuntijan tehtävä eduskunnan oikeusasiamiehen kutsumana.
Anita Puustjärvi: Sivutoimet: asiantuntijalääkäri, Kela, Itäinen vakuutuspiiri; työnohjaaja, useita työnantajia. Koulutustoiminta: Suomen Lastenpsykiatriyhdistys ry, Suomen Lääkäriliitto, Suomen koulu- ja opiskeluterveyden yhdistys Skooppi ry. Opetushallitus, yksittäisiä koulutuksia järjestäneet yliopistot, ammattikorkeakoulut ja opistot, ADHD-liitto, Live-säätiö, Valmennuskeskus Voimavara Oy, Siria Koulutus- ja kehittämiskeskus Oy, Cairos Coaching Oy, Takeda Oy, Biocodex Oy, Pharma Health Intelligence Oy (Lääketietokeskus). Luottamustoimet terveydenhuollon alalla: Suomen Lastenpsykiatriyhdistyksen koulutustoimikunta, puheenjohtaja 2009–2022, jäsen 2022–, johtokunta 2022–. Muut sidonnaisuudet: Julkaisu-/tekijänpalkkiot: Santalahti-kustannus, Duodecim, Otava.
Maria Sumia: Luottamustoimet terveydenhuollon alalla: Suomen Efcap ry, koulutustoimikunta.
Maarit Virta-Jämiä: Koulutustoiminta: Helsingin yliopisto, Tieteellinen hypnoosi ry, Hogrefe Psykologien kustannus, Mehiläinen, KAT ry, Suomen Neuropsykologinen yhdistys, Suomen Neuropsykoterapiayhdistys ry, Tampereen yliopisto, Integrum-instituutti, HUS, Helsingin kaupunki. Muut sidonnaisuudet: Resolvo Oy (yksityinen terveydenhuollon yritys): omistaja 50 %. Julkaisu-/tekijänoikeuspalkkiot: Tammi, Hogrefe Psykologien kustannus Oy, Kustannus Oy Duodecim.
Kirjallisuusviite
ADHD (aktiivisuuden ja tarkkaavuuden häiriö). Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin, Suomen Lastenneurologisen yhdistys ry:n, Suomen Lastenpsykiatriyhdistyksen ja Suomen Nuorisopsykiatrisen yhdistyksen asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2025 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
Tarkemmat viittausohjeet: «http://www.kaypahoito.fi/web/kh/viittaaminen»17
Vastuun rajaus
Käypä hoito -suositukset ja Vältä viisaasti -suositukset ovat asiantuntijoiden laatimia yhteenvetoja yksittäisten sairauksien diagnostiikan ja hoidon vaikuttavuudesta. Suositukset toimivat lääkärin tai muun terveydenhuollon ammattilaisen päätöksenteon tukena hoitopäätöksiä tehtäessä. Ne eivät korvaa lääkärin tai muun terveydenhuollon ammattilaisen omaa arviota yksittäisen potilaan parhaasta mahdollisesta diagnostiikasta, hoidosta ja kuntoutuksesta hoitopäätöksiä tehtäessä.
Tiedonhakukäytäntö
Systemaattinen kirjallisuushaku on hoitosuosituksen perusta. Lue lisää artikkelista khk00007
Kirjallisuutta
- Danielson J, Mohammadi N, Espinosa-Leal L. Attention Deficit Hyperactivity Disorder: trends and themes of information seeking and needs. INF [Internet]. 17. joulukuuta 2024 [viitattu 9. huhtikuuta 2025];43(3-4):74-80. Saatavissa: https://journal.fi/inf/article/view/148580
- Ayano G, Demelash S, Gizachew Y, ym. The global prevalence of attention deficit hyperactivity disorder in children and adolescents: An umbrella review of meta-analyses. J Affect Disord 2023;339():860-866 «PMID: 37495084»PubMed
- Salari N, Ghasemi H, Abdoli N, ym. The global prevalence of ADHD in children and adolescents: a systematic review and meta-analysis. Ital J Pediatr 2023;49(1):48 «PMID: 37081447»PubMed
- Polanczyk GV, Willcutt EG, Salum GA, ym. ADHD prevalence estimates across three decades: an updated systematic review and meta-regression analysis. Int J Epidemiol 2014;43(2):434-42 «PMID: 24464188»PubMed
- Polanczyk GV, Salum GA, Sugaya LS, ym. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry 2015;56(3):345-65 «PMID: 25649325»PubMed
- Thomas R, Sanders S, Doust J, ym. Prevalence of attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Pediatrics 2015;135(4):e994-1001 «PMID: 25733754»PubMed
- Vuori M, Paavilainen M, Vuorenmaa M, Tuovinen E, Aalto-Setälä T. Lasten ja nuorten ADHD-diagnoosien yleisyys 2023. ADHD-diagnoosit yleistyvät edelleen – sukupuolierot kaventuvat erityisesti nuoruusikäisessä väestössä. THL tilastoraportti 4/2025. 11.3.2025, https://www.julkari.fi/handle/10024/151005
- Fayyad J, De Graaf R, Kessler R, ym. Cross-national prevalence and correlates of adult attention-deficit hyperactivity disorder. Br J Psychiatry 2007;190():402-9 «PMID: 17470954»PubMed
- Fayyad J, Sampson NA, Hwang I, ym. The descriptive epidemiology of DSM-IV Adult ADHD in the World Health Organization World Mental Health Surveys. Atten Defic Hyperact Disord 2017;9(1):47-65 «PMID: 27866355»PubMed
- Song P, Zha M, Yang Q, ym. The prevalence of adult attention-deficit hyperactivity disorder: A global systematic review and meta-analysis. J Glob Health 2021;11():04009 «PMID: 33692893»PubMed
- Faraone SV, Banaschewski T, Coghill D, ym. The World Federation of ADHD International Consensus Statement: 208 Evidence-based conclusions about the disorder. Neurosci Biobehav Rev 2021;128():789-818 «PMID: 33549739»PubMed
- Dobrosavljevic M, Solares C, Cortese S, ym. Prevalence of attention-deficit/hyperactivity disorder in older adults: A systematic review and meta-analysis. Neurosci Biobehav Rev 2020;118():282-289 «PMID: 32798966»PubMed
- Auro K, Holopainen I, Perola M, ym. Attention-Deficit/Hyperactivity Disorder Diagnoses in Finland During the COVID-19 Pandemic. JAMA Netw Open 2024;7(6):e2418204 «PMID: 38935377»PubMed
- Sibley MH, Mitchell JT, Becker SP. Method of adult diagnosis influences estimated persistence of childhood ADHD: a systematic review of longitudinal studies. Lancet Psychiatry 2016;3(12):1157-1165 «PMID: 27745869»PubMed
- Simon V, Czobor P, Bálint S, ym. Prevalence and correlates of adult attention-deficit hyperactivity disorder: meta-analysis. Br J Psychiatry 2009;194(3):204-11 «PMID: 19252145»PubMed
- Joelsson P, Chudal R, Gyllenberg D, ym. Demographic Characteristics and Psychiatric Comorbidity of Children and Adolescents Diagnosed with ADHD in Specialized Healthcare. Child Psychiatry Hum Dev 2016;47(4):574-82 «PMID: 26399420»PubMed
- Polanczyk G, de Lima MS, Horta BL, ym. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry 2007;164(6):942-8 «PMID: 17541055»PubMed
- Ramtekkar UP, Reiersen AM, Todorov AA, ym. Sex and age differences in attention-deficit/hyperactivity disorder symptoms and diagnoses: implications for DSM-V and ICD-11. J Am Acad Child Adolesc Psychiatry 2010;49(3):217-28.e1-3 «PMID: 20410711»PubMed
- Rucklidge JJ. Gender differences in attention-deficit/hyperactivity disorder. Psychiatr Clin North Am 2010;33(2):357-73 «PMID: 20385342»PubMed
- Skoglund C, Sundström Poromaa I, Leksell D, ym. Time after time: failure to identify and support females with ADHD - a Swedish population register study. J Child Psychol Psychiatry 2024;65(6):832-844 «PMID: 38016697»PubMed
- Adamis D, Flynn C, Wrigley M, ym. ADHD in Adults: A Systematic Review and Meta-Analysis of Prevalence Studies in Outpatient Psychiatric Clinics. J Atten Disord 2022;26(12):1523-1534 «PMID: 35373645»PubMed
- Whitely M, Raven M, Timimi S, ym. Attention deficit hyperactivity disorder late birthdate effect common in both high and low prescribing international jurisdictions: a systematic review. J Child Psychol Psychiatry 2019;60(4):380-391 «PMID: 30317644»PubMed
- Vuori M, Martikainen JE, Koski-Pirilä A, ym. Children's Relative Age and ADHD Medication Use: A Finnish Population-Based Study. Pediatrics 2020;146(4): «PMID: 32958613»PubMed
- Vuori M, Vuorenmaa M, Ervasti E, Tuovinen E, Aalto-Setälä T. Lasten ja nuorten ADHD-diagnoosien yleisyys 2022. ADHD-diagnoosit yleistyvät tasaisesti – sukupuoli- ja alue-erot ovat melko suuria. THL Tilastoraportti 1/2024, 23.1.2024, https://urn.fi/URN:NBN:fi-fe202401183216
- Kazda L, Bell K, Thomas R, ym. Attention deficit/hyperactivity disorder (ADHD) in children: more focus on care and support, less on diagnosis. BMJ 2024;384():e073448 «PMID: 38325889»PubMed
- Westman E, Prami T, Kallio A, ym. Increase in Occurrence of Attention Deficit Hyperactivity Disorder Differs by Age Group and Gender-Finnish Nationwide Register Study. Brain Behav 2025;15(1):e70253 «PMID: 39829159»PubMed
- Montagni I, Guichard E, Kurth T. Association of screen time with self-perceived attention problems and hyperactivity levels in French students: a cross-sectional study. BMJ Open 2016;6(2):e009089 «PMID: 26920440»PubMed
- Ra CK, Cho J, Stone MD, ym. Association of Digital Media Use With Subsequent Symptoms of Attention-Deficit/Hyperactivity Disorder Among Adolescents. JAMA 2018;320(3):255-263 «PMID: 30027248»PubMed
- Yeung A, Ng E, Abi-Jaoude E. TikTok and Attention-Deficit/Hyperactivity Disorder: A Cross-Sectional Study of Social Media Content Quality. Can J Psychiatry 2022;67(12):899-906 «PMID: 35196157»PubMed
- Verma S, Sinha SK. How evidence-based is the "hashtag ADHD test" (#adhdtest). A cross-sectional content analysis of TikTok videos on attention-deficit/hyperactivity disorder (ADHD) screening. Australas Psychiatry 2025;33(1):82-88 «PMID: 39422639»PubMed
- Faraone SV, Larsson H. Genetics of attention deficit hyperactivity disorder. Mol Psychiatry 2019;24(4):562-575 «PMID: 29892054»PubMed
- Sonuga-Barke EJS, Becker SP, Bölte S, ym. Annual Research Review: Perspectives on progress in ADHD science - from characterization to cause. J Child Psychol Psychiatry 2023;64(4):506-532 «PMID: 36220605»PubMed
- Thapar A, Cooper M. Attention deficit hyperactivity disorder. Lancet 2016;387(10024):1240-50 «PMID: 26386541»PubMed
- Nigg J, Nikolas M, Burt SA. Measured gene-by-environment interaction in relation to attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 2010;49(9):863-73 «PMID: 20732623»PubMed
- van der Meer D, Hoekstra PJ, Bralten J, ym. Interplay between stress response genes associated with attention-deficit hyperactivity disorder and brain volume. Genes Brain Behav 2016;15(7):627-36 «PMID: 27391809»PubMed
- Chen Q, Brikell I, Lichtenstein P, ym. Familial aggregation of attention-deficit/hyperactivity disorder. J Child Psychol Psychiatry 2017;58(3):231-239 «PMID: 27545745»PubMed
- Brikell I, Burton C, Mota NR, ym. Insights into attention-deficit/hyperactivity disorder from recent genetic studies. Psychol Med 2021;51(13):2274-2286 «PMID: 33814023»PubMed
- Ribasés M, Mitjans M, Hartman CA, ym. Genetic architecture of ADHD and overlap with other psychiatric disorders and cognition-related phenotypes. Neurosci Biobehav Rev 2023;153():105313 «PMID: 37451654»PubMed
- Demontis D, Walters GB, Athanasiadis G, ym. Genome-wide analyses of ADHD identify 27 risk loci, refine the genetic architecture and implicate several cognitive domains. Nat Genet 2023;55(2):198-208 «PMID: 36702997»PubMed
- Cole J, Ball HA, Martin NC, ym. Genetic overlap between measures of hyperactivity/inattention and mood in children and adolescents. J Am Acad Child Adolesc Psychiatry 2009;48(11):1094-1101 «PMID: 19797986»PubMed
- Thapar A, Cooper M, Eyre O, ym. What have we learnt about the causes of ADHD? J Child Psychol Psychiatry 2013;54(1):3-16 «PMID: 22963644»PubMed
- Cross-Disorder Group of the Psychiatric Genomics Consortium. Identification of risk loci with shared effects on five major psychiatric disorders: a genome-wide analysis. Lancet 2013;381(9875):1371-1379 «PMID: 23453885»PubMed
- Thapar A. Discoveries on the Genetics of ADHD in the 21st Century: New Findings and Their Implications. Am J Psychiatry 2018;175(10):943-950 «PMID: 30111187»PubMed
- Andersson A, Tuvblad C, Chen Q, ym. Research Review: The strength of the genetic overlap between ADHD and other psychiatric symptoms - a systematic review and meta-analysis. J Child Psychol Psychiatry 2020;61(11):1173-1183 «PMID: 32157695»PubMed
- Kittel-Schneider S, Arteaga-Henriquez G, Vasquez AA, ym. Non-mental diseases associated with ADHD across the lifespan: Fidgety Philipp and Pippi Longstocking at risk of multimorbidity? Neurosci Biobehav Rev 2022;132():1157-1180 «PMID: 34757108»PubMed
- Grimm O, Kranz TM, Reif A. Genetics of ADHD: What Should the Clinician Know? Curr Psychiatry Rep 2020;22(4):18 «PMID: 32108282»PubMed
- Grimm O, Kittel-Schneider S, Reif A. Recent developments in the genetics of attention-deficit hyperactivity disorder. Psychiatry Clin Neurosci 2018;72(9):654-672 «PMID: 29722101»PubMed
- Smith TF, Schmidt-Kastner R, McGeary JE, ym. Pre- and Perinatal Ischemia-Hypoxia, the Ischemia-Hypoxia Response Pathway, and ADHD Risk. Behav Genet 2016;46(3):467-77 «PMID: 26920003»PubMed
- Bitsko RH, Holbrook JR, O'Masta B, ym. A Systematic Review and Meta-analysis of Prenatal, Birth, and Postnatal Factors Associated with Attention-Deficit/Hyperactivity Disorder in Children. Prev Sci 2024;25(Suppl 2):203-224 «PMID: 35303250»PubMed
- Robinson R, Girchenko P, Pulakka A, ym. ADHD symptoms and diagnosis in adult preterms: systematic review, IPD meta-analysis, and register-linkage study. Pediatr Res 2023;93(5):1399-1409 «PMID: 34997222»PubMed
- Neuman RJ, Lobos E, Reich W, ym. Prenatal smoking exposure and dopaminergic genotypes interact to cause a severe ADHD subtype. Biol Psychiatry 2007;61(12):1320-8 «PMID: 17157268»PubMed
- Joelsson P, Chudal R, Talati A, ym. Prenatal smoking exposure and neuropsychiatric comorbidity of ADHD: a finnish nationwide population-based cohort study. BMC Psychiatry 2016;16(1):306 «PMID: 27581195»PubMed
- Langley K, Rice F, van den Bree MB, ym. Maternal smoking during pregnancy as an environmental risk factor for attention deficit hyperactivity disorder behaviour. A review. Minerva Pediatr 2005;57(6):359-71 «PMID: 16402008»PubMed
- Biederman J, Petty CR, Bhide PG, ym. Does exposure to maternal smoking during pregnancy affect the clinical features of ADHD? Results from a controlled study. World J Biol Psychiatry 2012;13(1):60-4 «PMID: 21545244»PubMed
- Haan E, Westmoreland KE, Schellhas L, ym. Prenatal smoking, alcohol and caffeine exposure and offspring externalizing disorders: a systematic review and meta-analysis. Addiction 2022;117(10):2602-2613 «PMID: 35385887»PubMed
- Huang L, Wang Y, Zhang L, ym. Maternal Smoking and Attention-Deficit/Hyperactivity Disorder in Offspring: A Meta-analysis. Pediatrics 2018;141(1): «PMID: 29288161»PubMed
- Nygaard E, Slinning K, Moe V, ym. Behavior and Attention Problems in Eight-Year-Old Children with Prenatal Opiate and Poly-Substance Exposure: A Longitudinal Study. PLoS One 2016;11(6):e0158054 «PMID: 27336798»PubMed
- Knopik VS, Sparrow EP, Madden PA, ym. Contributions of parental alcoholism, prenatal substance exposure, and genetic transmission to child ADHD risk: a female twin study. Psychol Med 2005;35(5):625-35 «PMID: 15918339»PubMed
- Brookes KJ, Mill J, Guindalini C, ym. A common haplotype of the dopamine transporter gene associated with attention-deficit/hyperactivity disorder and interacting with maternal use of alcohol during pregnancy. Arch Gen Psychiatry 2006;63(1):74-81 «PMID: 16389200»PubMed
- Han JY, Kwon HJ, Ha M, ym. The effects of prenatal exposure to alcohol and environmental tobacco smoke on risk for ADHD: a large population-based study. Psychiatry Res 2015;225(1-2):164-168 «PMID: 25481018»PubMed
- Ackerman JP, Riggins T, Black MM. A review of the effects of prenatal cocaine exposure among school-aged children. Pediatrics 2010;125(3):554-65 «PMID: 20142293»PubMed
- Noland JS, Singer LT, Short EJ, ym. Prenatal drug exposure and selective attention in preschoolers. Neurotoxicol Teratol 2005;27(3):429-38 «PMID: 15939203»PubMed
- Huizink AC, Mulder EJ. Maternal smoking, drinking or cannabis use during pregnancy and neurobehavioral and cognitive functioning in human offspring. Neurosci Biobehav Rev 2006;30(1):24-41 «PMID: 16095697»PubMed
- Elgen I, Bruaroy S, Laegreid LM. Complexity of foetal alcohol or drug neuroimpairments. Acta Paediatr 2007;96(12):1730-3 «PMID: 17971190»PubMed
- Li L, Lagerberg T, Chang Z, ym. Maternal pre-pregnancy overweight/obesity and the risk of attention-deficit/hyperactivity disorder in offspring: a systematic review, meta-analysis and quasi-experimental family-based study. Int J Epidemiol 2020;49(3):857-875 «PMID: 32337582»PubMed
- Nilsson IAK, Ozsvar J, Gissler M, ym. Maternal Eating Disorders, Body Mass Index, and Offspring Psychiatric Diagnoses. JAMA Netw Open 2024;7(10):e2440517 «PMID: 39436646»PubMed
- Duko B, Mengistu TS, Stacey D, ym. Associations between maternal preconception and pregnancy adiposity and neuropsychiatric and behavioral outcomes in the offspring: A systematic review and meta-analysis. Psychiatry Res 2024;342():116149 «PMID: 39278191»PubMed
- Van den Bergh BRH, van den Heuvel MI, Lahti M, ym. Prenatal developmental origins of behavior and mental health: The influence of maternal stress in pregnancy. Neurosci Biobehav Rev 2020;117():26-64 «PMID: 28757456»PubMed
- Okano L, Ji Y, Riley AW, ym. Maternal psychosocial stress and children's ADHD diagnosis: a prospective birth cohort study. J Psychosom Obstet Gynaecol 2019;40(3):217-225 «PMID: 29790815»PubMed
- Jallow J, Hurtig T, Kerkelä M, ym. Prenatal maternal stress, breastfeeding and offspring ADHD symptoms. Eur Child Adolesc Psychiatry 2024;33(11):4003-4011 «PMID: 38691181»PubMed
- Humphreys KL, Zeanah CH. Deviations from the expectable environment in early childhood and emerging psychopathology. Neuropsychopharmacology 2015;40(1):154-70 «PMID: 24998622»PubMed
- Golm D, Sarkar S, Mackes NK, ym. The impact of childhood deprivation on adult neuropsychological functioning is associated with ADHD symptom persistence. Psychol Med 2021;51(15):2675-2684 «PMID: 32419675»PubMed
- Wylock JF, Borghini A, Slama H, ym. Child attachment and ADHD: a systematic review. Eur Child Adolesc Psychiatry 2023;32(1):5-16 «PMID: 33844103»PubMed
- Storebø OJ, Rasmussen PD, Simonsen E. Association Between Insecure Attachment and ADHD: Environmental Mediating Factors. J Atten Disord 2016;20(2):187-96 «PMID: 24062279»PubMed
- Al-Yagon M, Forte D, Avrahami L. Executive Functions and Attachment Relationships in Children With ADHD: Links to Externalizing/Internalizing Problems, Social Skills, and Negative Mood Regulation. J Atten Disord 2020;24(13):1876-1890 «PMID: 28918685»PubMed
- Pallini S, Morelli M, Chirumbolo A, ym. Attachment and attention problems: A meta-analysis. Clin Psychol Rev 2019;74():101772 «PMID: 31739122»PubMed
- Claussen AH, Holbrook JR, Hutchins HJ, ym. All in the Family? A Systematic Review and Meta-analysis of Parenting and Family Environment as Risk Factors for Attention-Deficit/Hyperactivity Disorder (ADHD) in Children. Prev Sci 2024;25(Suppl 2):249-271 «PMID: 35438451»PubMed
- Deault LC. A systematic review of parenting in relation to the development of comorbidities and functional impairments in children with attention-deficit/hyperactivity disorder (ADHD). Child Psychiatry Hum Dev 2010;41(2):168-92 «PMID: 19768532»PubMed
- Park JL, Hudec KL, Johnston C. Parental ADHD symptoms and parenting behaviors: A meta-analytic review. Clin Psychol Rev 2017;56():25-39 «PMID: 28601690»PubMed
- Robinson LR, Bitsko RH, O'Masta B, ym. A Systematic Review and Meta-analysis of Parental Depression, Antidepressant Usage, Antisocial Personality Disorder, and Stress and Anxiety as Risk Factors for Attention-Deficit/Hyperactivity Disorder (ADHD) in Children. Prev Sci 2024;25(Suppl 2):272-290 «PMID: 35641729»PubMed
- Niiranen J, Kiviruusu O, Vornanen R, ym. Children's screen time and psychosocial symptoms at 5 years of age - the role of parental factors. BMC Pediatr 2024;24(1):500 «PMID: 39097686»PubMed
- Radesky JS, Kaciroti N, Weeks HM, ym. Longitudinal Associations Between Use of Mobile Devices for Calming and Emotional Reactivity and Executive Functioning in Children Aged 3 to 5 Years. JAMA Pediatr 2023;177(1):62-70 «PMID: 36508199»PubMed
- Anitha FS, Narasimhan U, Janakiraman A, ym. Association of digital media exposure and addiction with child development and behavior: A cross-sectional study. Ind Psychiatry J 2021;30(2):265-271 «PMID: 35017810»PubMed
- Girela-Serrano BM, Spiers ADV, Ruotong L, ym. Impact of mobile phones and wireless devices use on children and adolescents' mental health: a systematic review. Eur Child Adolesc Psychiatry 2024;33(6):1621-1651 «PMID: 35705765»PubMed
- Guidelines on physical activity, sedentary behaviour and sleep for children under 5 years of age. Geneva: World Health Organization; 2019. Licence: CC BY-NC-SA 3.0 IGO. https://iris.who.int/bitstream/handle/10665/311664/9789241550536-eng.pdf?sequence
- Lederer Y, Artzi H, Borodkin K. The effects of maternal smartphone use on mother-child interaction. Child Dev 2022;93(2):556-570 «PMID: 34807453»PubMed
- Kosola S. Lasten ja nuorten netti- ja peliriippuvuus: pitääkö olla huolissaan? Suom Lääkäril 2020;6:324-9
- Dekkers TJ, van Hoorn J. Understanding Problematic Social Media Use in Adolescents with Attention-Deficit/Hyperactivity Disorder (ADHD): A Narrative Review and Clinical Recommendations. Brain Sci 2022;12(12): «PMID: 36552085»PubMed
- Christensen MA, Bettencourt L, Kaye L, ym. Direct Measurements of Smartphone Screen-Time: Relationships with Demographics and Sleep. PLoS One 2016;11(11):e0165331 «PMID: 27829040»PubMed
- Ferguson CK, Branley-Bell D, ym. Screen Media and Mental Health. Professional psychology, research and practice 2022;53:205-14
- Nan YQ, Li Z, ym. Is Social Media Use Related to Social Anxiety? A Meta–Analysis. . Mass communication & society 2024;27:441-74
- Liebherr MS, Antons S, Montag C, Brand M. Smartphones and attention, curse or blessing? - A review on the effects of smartphone usage on attention, inhibition, and working memory. Computers in Human Behavior Reports 2020;1:1-8
- Rubia K, Alegría AA, Brinson H. Brain abnormalities in attention-deficit hyperactivity disorder: a review. Rev Neurol 2014;58 Suppl 1():S3-16 «PMID: 25252664»PubMed
- Nakao T, Radua J, Rubia K, ym. Gray matter volume abnormalities in ADHD: voxel-based meta-analysis exploring the effects of age and stimulant medication. Am J Psychiatry 2011;168(11):1154-63 «PMID: 21865529»PubMed
- Frodl T, Skokauskas N. Meta-analysis of structural MRI studies in children and adults with attention deficit hyperactivity disorder indicates treatment effects. Acta Psychiatr Scand 2012;125(2):114-26 «PMID: 22118249»PubMed
- Spencer TJ, Brown A, Seidman LJ, ym. Effect of psychostimulants on brain structure and function in ADHD: a qualitative literature review of magnetic resonance imaging-based neuroimaging studies. J Clin Psychiatry 2013;74(9):902-17 «PMID: 24107764»PubMed
- Hoogman M, Bralten J, Hibar DP, ym. Subcortical brain volume differences in participants with attention deficit hyperactivity disorder in children and adults: a cross-sectional mega-analysis. Lancet Psychiatry 2017;4(4):310-319 «PMID: 28219628»PubMed
- Hoogman M, Muetzel R, Guimaraes JP, ym. Brain Imaging of the Cortex in ADHD: A Coordinated Analysis of Large-Scale Clinical and Population-Based Samples. Am J Psychiatry 2019;176(7):531-542 «PMID: 31014101»PubMed
- Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med 2006;36(2):159-65 «PMID: 16420712»PubMed
- Kessler RC, Green JG, Adler LA, ym. Structure and diagnosis of adult attention-deficit/hyperactivity disorder: analysis of expanded symptom criteria from the Adult ADHD Clinical Diagnostic Scale. Arch Gen Psychiatry 2010;67(11):1168-78 «PMID: 21041618»PubMed
- Graziano PA, Garcia A. Attention-deficit hyperactivity disorder and children's emotion dysregulation: A meta-analysis. Clin Psychol Rev 2016;46():106-23 «PMID: 27180913»PubMed
- Corbisiero S, Mörstedt B, Bitto H, ym. Emotional Dysregulation in Adults With Attention-Deficit/Hyperactivity Disorder-Validity, Predictability, Severity, and Comorbidity. J Clin Psychol 2017;73(1):99-112 «PMID: 27153511»PubMed
- Vuori M, Autti-Rämö I, Junttila N, ym. Discrepancies between self- and adult-perceptions of social competence in children with neuropsychiatric disorders. Child Care Health Dev 2017;43(5):670-678 «PMID: 27644170»PubMed
- Shaw P, Stringaris A, Nigg J, ym. Emotion dysregulation in attention deficit hyperactivity disorder. Am J Psychiatry 2014;171(3):276-93 «PMID: 24480998»PubMed
- Findon JL, Muck A, Tóthpál-Davison B, ym. Investigating behavioural addictions in adults with and without attention deficit hyperactivity disorder. PLoS One 2025;20(2):e0317525 «PMID: 39908223»PubMed
- Rahapeliongelma. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Päihdelääketieteen yhdistyksen asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2023 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Young S, Uysal O, Kahle J, ym. A systematic review and meta-analysis comparing the severity of core symptoms of attention-deficit hyperactivity disorder in females and males. Psychol Med 2024;54(14):1-22 «PMID: 39494848»PubMed
- Eng AG, Nirjar U, Elkins AR, ym. Attention-deficit/hyperactivity disorder and the menstrual cycle: Theory and evidence. Horm Behav 2024;158():105466 «PMID: 38039899»PubMed
- Bürger I, Erlandsson K, Borneskog C. Perceived associations between the menstrual cycle and Attention Deficit Hyperactivity Disorder (ADHD): A qualitative interview study exploring lived experiences. Sex Reprod Healthc 2024;40():100975 «PMID: 38678676»PubMed
- Camara B, Padoin C, Bolea B. Relationship between sex hormones, reproductive stages and ADHD: a systematic review. Arch Womens Ment Health 2022;25(1):1-8 «PMID: 34487213»PubMed
- Onandia-Hinchado I, Pardo-Palenzuela N, Diaz-Orueta U. Cognitive characterization of adult attention deficit hyperactivity disorder by domains: a systematic review. J Neural Transm (Vienna) 2021;128(7):893-937 «PMID: 33620582»PubMed
- Frazier TW, Demaree HA, Youngstrom EA. Meta-analysis of intellectual and neuropsychological test performance in attention-deficit/hyperactivity disorder. Neuropsychology 2004;18(3):543-55 «PMID: 15291732»PubMed
- Sadozai AK, Sun C, Demetriou EA, ym. Executive function in children with neurodevelopmental conditions: a systematic review and meta-analysis. Nat Hum Behav 2024;8(12):2357-2366 «PMID: 39424962»PubMed
- Boonstra AM, Oosterlaan J, Sergeant JA, ym. Executive functioning in adult ADHD: a meta-analytic review. Psychol Med 2005;35(8):1097-108 «PMID: 16116936»PubMed
- Alderson RM, Kasper LJ, Hudec KL, ym. Attention-deficit/hyperactivity disorder (ADHD) and working memory in adults: a meta-analytic review. Neuropsychology 2013;27(3):287-302 «PMID: 23688211»PubMed
- Ramos AA, Hamdan AC, Machado L. A meta-analysis on verbal working memory in children and adolescents with ADHD. Clin Neuropsychol 2020;34(5):873-898 «PMID: 31007130»PubMed
- Kooij JJS, Bijlenga D, Salerno L, ym. Updated European Consensus Statement on diagnosis and treatment of adult ADHD. Eur Psychiatry 2019;56():14-34 «PMID: 30453134»PubMed
- Coghill D, Banaschewski T, Cortese S, ym. The management of ADHD in children and adolescents: bringing evidence to the clinic: perspective from the European ADHD Guidelines Group (EAGG). Eur Child Adolesc Psychiatry 2023;32(8):1337-1361 «PMID: 34677682»PubMed
- Mulraney M, Arrondo G, Musullulu H, ym. Systematic Review and Meta-analysis: Screening Tools for Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. J Am Acad Child Adolesc Psychiatry 2022;61(8):982-996 «PMID: 34958872»PubMed
- Marshall P, Hoelzle J, Nikolas M. Diagnosing Attention-Deficit/Hyperactivity Disorder (ADHD) in young adults: A qualitative review of the utility of assessment measures and recommendations for improving the diagnostic process. Clin Neuropsychol 2021;35(1):165-198 «PMID: 31791193»PubMed
- Eom TH, Kim YH. Clinical practice guidelines for attention-deficit/hyperactivity disorder: recent updates. Clin Exp Pediatr 2024;67(1):26-34 «PMID: 37321571»PubMed
- National Guideline Centre (UK). Attention deficit hyperactivity disorder: diagnosis and management. NICE Guideline, No. 87. London: National Institute for Health and Care Excellence (UK), 2018.
- Barbaresi WJ, Campbell L, Diekroger EA, ym. The Society for Developmental and Behavioral Pediatrics Clinical Practice Guideline for the Assessment and Treatment of Children and Adolescents with Complex Attention-Deficit/Hyperactivity Disorder: Process of Care Algorithms. J Dev Behav Pediatr 2020;41 Suppl 2S():S58-S74 «PMID: 31996578»PubMed
- AADPA. Australian Evidence-Based Clinical Practice Guideline For Attention Deficit Hyperactivity Disorder (ADHD). 2022,https://adhdguideline.aadpa.com.au.
- Penttilä S, Niemelä M, Hakko H, ym. Child- and parent-related determinants for out-of-home care in a nationwide population with neurodevelopmental disorders: a register-based Finnish birth cohort 1997 study. Eur Child Adolesc Psychiatry 2024;33(10):3459-3470 «PMID: 38430236»PubMed
- Lehti V, Chudal R, Suominen A, ym. Association between immigrant background and ADHD: a nationwide population-based case-control study. J Child Psychol Psychiatry 2016;57(8):967-75 «PMID: 27133554»PubMed
- Caye A, Rocha TB, Anselmi L, ym. Attention-Deficit/Hyperactivity Disorder Trajectories From Childhood to Young Adulthood: Evidence From a Birth Cohort Supporting a Late-Onset Syndrome. JAMA Psychiatry 2016;73(7):705-12 «PMID: 27192050»PubMed
- Agnew-Blais JC, Polanczyk GV, Danese A, ym. Evaluation of the Persistence, Remission, and Emergence of Attention-Deficit/Hyperactivity Disorder in Young Adulthood. JAMA Psychiatry 2016;73(7):713-20 «PMID: 27192174»PubMed
- Moffitt TE, Houts R, Asherson P, ym. Is Adult ADHD a Childhood-Onset Neurodevelopmental Disorder? Evidence From a Four-Decade Longitudinal Cohort Study. Am J Psychiatry 2015;172(10):967-77 «PMID: 25998281»PubMed
- The World Health Organization (WHO). International Classification of Diseases Eleventh Revision (ICD-11). Geneva: World Health Organization; 2022. https://icd.who.int/en
- Peterson BS, Trampush J, Brown M, ym. Tools for the Diagnosis of ADHD in Children and Adolescents: A Systematic Review. Pediatrics 2024;153(4): «PMID: 38523599»PubMed
- Harrison AG, Edwards MJ. The Ability of Self-Report Methods to Accurately Diagnose Attention Deficit Hyperactivity Disorder: A Systematic Review. J Atten Disord 2023;27(12):1343-1359 «PMID: 37366274»PubMed
- Arrondo G, Mulraney M, Iturmendi-Sabater I, ym. Systematic Review and Meta-Analysis: Clinical Utility of Continuous Performance Tests for the Identification of Attention-Deficit/Hyperactivity Disorder. J Am Acad Child Adolesc Psychiatry 2024;63(2):154-171 «PMID: 37004919»PubMed
- Caselles-Pina L, Quesada-López A, Sújar A, ym. A systematic review on the application of machine learning models in psychometric questionnaires for the diagnosis of attention deficit hyperactivity disorder. Eur J Neurosci 2024;60(3):4115-4127 «PMID: 38378245»PubMed
- Sawaya H, Miller JC, Raines JM. Review of Studies on Incremental Validity of Assessment Measures Used in Psychological Assessment of Attention-Deficit Hyperactivity Disorder. Assessment 2024;31(2):518-537 «PMID: 36914964»PubMed
- Korkeila J, Leppämäki S, Virta M. Aktiivisuuden ja tarkkaavuuden häiriö (ADHD). Teoksessa: Juva K, Hublin C, Kalska H, Korkeila J, Sainio M, Tani P ja Vataja R (toim). Kliininen neuropsykiatria. Kustannus Oy Duodecim 2021, 733 p.
- Aivovammat. Suomalaisen Lääkäriseuran Duodecimin, Suomen Neurologisen yhdistys ry:n, Societas Medicinae Physicalis et Rehabilitationis Fenniae ry:n, Suomen Neurokirurgisen yhdistyksen, Suomen Neuropsykologisen yhdistyksen ja Suomen Vakuutuslääkärien yhdistyksen asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2023 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Kehityksellinen kielihäiriö (kielen kehityksen häiriö, lapset ja nuoret). Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin, Suomen Foniatrit ry:n ja Suomen Lastenneurologisen Yhdistyksen asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2019 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Lasten ja nuorten kehityksellinen koordinaatiohäiriö (DCD). Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Lastenneurologinen Yhdistys ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Autismikirjon häiriö. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Lastenpsykiatriyhdistyksen, Suomen Nuorisopsykiatrisen Yhdistyksen, Suomen Kehitysvammalääkäreiden, Suomen Lastenneurologisen Yhdistyksen ja Suomen Psykiatriyhdistyksen asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Käytöshäiriöt (lapset ja nuoret). Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin, Suomen lastenpsykiatriyhdistyksen, Suomen nuorisopsykiatrisen yhdistyksen ja Suomen Psykiatriyhdistyksen Nuorisopsykiatrian jaoksen asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2018 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Ahdistuneisuushäiriöt. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin, Suomen Psykiatriyhdistys ry:n ja Suomen Nuorisopsykiatrisen yhdistyksen asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Pakko-oireinen häiriö. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin , Suomen Psykiatriyhdistys ry:n jaSuomen Lastenpsykiatriyhdistys ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2023 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Depressio. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Psykiatriyhdistys ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Kaksisuuntainen mielialahäiriö. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin, Suomen Psykiatriyhdistys ry:n ja Suomen Nuorisopsykiatrisen yhdistyksen asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Traumaperäinen stressihäiriö. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Psykiatriyhdistys ry:n ja Suomen Lastenpsykiatriyhdistys ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2022 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Epävakaa persoonallisuus. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Psykiatriyhdistys ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Alkoholiongelmat. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Päihdelääketieteen yhdistyksen asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2015 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Huumeongelmat. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Päihdelääketieteen yhdistyksen asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2022 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi [
- Skitsofrenia. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Psykiatriyhdistys ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
- Wolraich ML, Hagan JF Jr, Allan C, ym. Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics 2019;144(4): «PMID: 31570648»PubMed
- Mechler K, Banaschewski T, Hohmann S, ym. Evidence-based pharmacological treatment options for ADHD in children and adolescents. Pharmacol Ther 2022;230():107940 «PMID: 34174276»PubMed
- Chan E, Fogler JM, Hammerness PG. Treatment of Attention-Deficit/Hyperactivity Disorder in Adolescents: A Systematic Review. JAMA 2016;315(18):1997-2008 «PMID: 27163988»PubMed
- Torgersen T, Gjervan B, Lensing MB, ym. Optimal management of ADHD in older adults. Neuropsychiatr Dis Treat 2016;12():79-87 «PMID: 26811680»PubMed
- Sibley MH, Flores S, Murphy M, ym. Research Review: Pharmacological and non-pharmacological treatments for adolescents with attention deficit/hyperactivity disorder - a systematic review of the literature. J Child Psychol Psychiatry 2025;66(1):132-149 «PMID: 39370392»PubMed
- Dahl V, Spears AP, ym. Psychoeducation interventions for parents and teachers of children and adolescents with ADHD: A systematic review of the literature. Journal of Developmental and Physical Disabilities 2020;32:257-92
- Brown RT, Amler RW, Freeman WS, ym. Treatment of attention-deficit/hyperactivity disorder: overview of the evidence. Pediatrics 2005;115(6):e749-57 «PMID: 15930203»PubMed
- Vidal-Estrada R, Bosch-Munso R, Nogueira-Morais M, ym. Psychological treatment of attention deficit hyperactivity disorder in adults: a systematic review. Actas Esp Psiquiatr 2012;40(3):147-54 «PMID: 22723133»PubMed
- Young S, Khondoker M, Emilsson B, ym. Cognitive-behavioural therapy in medication-treated adults with attention-deficit/hyperactivity disorder and co-morbid psychopathology: a randomized controlled trial using multi-level analysis. Psychol Med 2015;45(13):2793-804 «PMID: 26022103»PubMed
- Philipsen A, Jans T, Graf E, ym. Effects of Group Psychotherapy, Individual Counseling, Methylphenidate, and Placebo in the Treatment of Adult Attention-Deficit/Hyperactivity Disorder: A Randomized Clinical Trial. JAMA Psychiatry 2015;72(12):1199-210 «PMID: 26536057»PubMed
- Young S, Amarasinghe JM. Practitioner review: Non-pharmacological treatments for ADHD: a lifespan approach. J Child Psychol Psychiatry 2010;51(2):116-33 «PMID: 19891745»PubMed
- Sosiaali- ja terveysministeriö. Valtakunnalliset lääkinnälliseen kuntoutukseen ohjaamisen perusteet 2022. Opas terveyden- ja sosiaalihuollon ammattilaisille ja kuntoutuksen parissa työskenteleville. Sosiaali- ja terveysministeriön julkaisuja 2022:17
- Riddle MA, Yershova K, Lazzaretto D, ym. The Preschool Attention-Deficit/Hyperactivity Disorder Treatment Study (PATS) 6-year follow-up. J Am Acad Child Adolesc Psychiatry 2013;52(3):264-278.e2 «PMID: 23452683»PubMed
- Vitiello B, Lazzaretto D, Yershova K, ym. Pharmacotherapy of the Preschool ADHD Treatment Study (PATS) Children Growing Up. J Am Acad Child Adolesc Psychiatry 2015;54(7):550-6 «PMID: 26088659»PubMed
- Bölte S, Mahdi S, Coghill D, ym. Standardised assessment of functioning in ADHD: consensus on the ICF Core Sets for ADHD. Eur Child Adolesc Psychiatry 2018;27(10):1261-1281 «PMID: 29435654»PubMed
- Bölte S, Alehagen L, Black MH, ym. Assessment of functioning in ADHD according to World Health Organization standards: First revision of the International Classification of Functioning, Disability and Health Core Sets. Dev Med Child Neurol 2024;66(9):1201-1214 «PMID: 38308443»PubMed
- de Schipper E, Lundequist A, Wilteus AL, ym. A comprehensive scoping review of ability and disability in ADHD using the International Classification of Functioning, Disability and Health-Children and Youth Version (ICF-CY). Eur Child Adolesc Psychiatry 2015;24(8):859-72 «PMID: 26036861»PubMed
- Puustjärvi A, Kallio-Laine K, Klintrup K ym. Tunnetko ADHD-potilaan etuudet? Suom Lääkäril 2023;33:1274-6
- Uchida M, Driscoll H, DiSalvo M, ym. Assessing the Magnitude of Risk for ADHD in Offspring of Parents with ADHD: A Systematic Literature Review and Meta-Analysis. J Atten Disord 2021;25(13):1943-1948 «PMID: 32830611»PubMed
- Theule J, Wiener J. Parenting Stress in Families of Children With ADHD: A Meta-Analysis. J Emot Behav Disord 2013;21:3-17
- Endo K, Stanyon D, Yamasaki S, ym. Self-Reported Maternal Parenting Stress From 9 m Is Longitudinally Associated With Child ADHD Symptoms at Age 12: Findings From a Population-Based Birth Cohort Study. Front Psychiatry 2022;13():806669 «PMID: 35573369»PubMed
- Johnston C, Mash EJ, Miller N, ym. Parenting in adults with attention-deficit/hyperactivity disorder (ADHD). Clin Psychol Rev 2012;32(4):215-28 «PMID: 22459785»PubMed
- Friedman LM, Dvorsky MR, McBurnett K, ym. Do Parents' ADHD Symptoms Affect Treatment for their Children? The Impact of Parental ADHD on Adherence to Behavioral Parent Training for Childhood ADHD. J Abnorm Child Psychol 2020;48(11):1425-1437 «PMID: 32813210»PubMed
- Wymbs BT, Canu WH, Sacchetti GM, ym. Adult ADHD and romantic relationships: What we know and what we can do to help. J Marital Fam Ther 2021;47(3):664-681 «PMID: 33421168»PubMed
- Webster-Stratton CH, Reid MJ, Beauchaine T. Combining parent and child training for young children with ADHD. J Clin Child Adolesc Psychol 2011;40(2):191-203 «PMID: 21391017»PubMed
- Chronis-Tuscano A, Wang CH, Woods KE, ym. Parent ADHD and Evidence-Based Treatment for Their Children: Review and Directions for Future Research. J Abnorm Child Psychol 2017;45(3):501-517 «PMID: 28025755»PubMed
- Flynn MM, Rosen PJ, Reese JS, ym. Examining the influence of irritability and ADHD on domains of parenting stress. Eur Child Adolesc Psychiatry 2023;32(2):353-366 «PMID: 34510265»PubMed
- Sellers R, Harold GT, Thapar A, ym. Examining the Role of Genetic Risk and Longitudinal Transmission Processes Underlying Maternal Parenting and Psychopathology and Children's ADHD Symptoms and Aggression: Utilizing the Advantages of a Prospective Adoption Design. Behav Genet 2020;50(4):247-262 «PMID: 32623545»PubMed
- Williamson D, Johnston C, Noyes A, ym. Attention-Deficit/Hyperactivity Disorder Symptoms in Mothers and Fathers: Family Level Interactions in Relation to Parenting. J Abnorm Child Psychol 2017;45(3):485-500 «PMID: 27909931»PubMed
- Wells KC, Chi TC, Hinshaw SP, ym. Treatment-related changes in objectively measured parenting behaviors in the multimodal treatment study of children with attention-deficit/hyperactivity disorder. J Consult Clin Psychol 2006;74(4):649-57 «PMID: 16881772»PubMed
- Mikami AY, Pfiffner LJ. Sibling relationships among children with ADHD. J Atten Disord 2008;11(4):482-92 «PMID: 17494830»PubMed
- Peasgood T, Bhardwaj A, Biggs K, ym. The impact of ADHD on the health and well-being of ADHD children and their siblings. Eur Child Adolesc Psychiatry 2016;25(11):1217-1231 «PMID: 27037707»PubMed
- King K, Alexander D, Seabi J. Siblings' Perceptions of Their ADHD-Diagnosed Sibling's Impact on the Family System. Int J Environ Res Public Health 2016;13(9): «PMID: 27649212»PubMed
- Schumann A, Vatne TM, Fjermestad KW. What challenges do siblings of children with chronic disorders express to their parents? A thematic analysis of 73 sibling-parent dialogues. J Pediatr Nurs 2024;76():91-98 «PMID: 38367476»PubMed
- Vacher C, Goujon A, Romo L, ym. Efficacy of psychosocial interventions for children with ADHD and emotion dysregulation: a systematic review. Psychiatry Res 2020;291():113151 «PMID: 32619822»PubMed
- Breaux R, Baweja R, Eadeh HM, ym. Systematic Review and Meta-analysis: Pharmacological and Nonpharmacological Interventions for Persistent Nonepisodic Irritability. J Am Acad Child Adolesc Psychiatry 2023;62(3):318-334 «PMID: 35714838»PubMed
- Storebø OJ, Elmose Andersen M, Skoog M, ym. Social skills training for attention deficit hyperactivity disorder (ADHD) in children aged 5 to 18 years. Cochrane Database Syst Rev 2019;6(6):CD008223 «PMID: 31222721»PubMed
- Perusopetuksen opetussuunnitelman perusteiden muutokset ja täydennykset 2010. Opetushallitus. Määräykset ja ohjeet 2011:20 http://www.oph.fi/download/132882_Perusopetuksen_opetussuunnitelman_perusteiden_muutokset_ja_taydennykset2010.pdf
- Battagliese G, Caccetta M, Luppino OI, ym. Cognitive-behavioral therapy for externalizing disorders: A meta-analysis of treatment effectiveness. Behav Res Ther 2015;75():60-71 «PMID: 26575979»PubMed
- Fabiano GA, Schatz NK, Aloe AM, Pelham WE, Jr., Smyth AC, Zhao X, et al. Comprehensive meta-analysis of attention-deficit/hyperactivity disorder psychosocial treatments investigated within between group studies. Review of Educational Research. 2021;91(5):718-60
- Tourjman V, Louis-Nascan G, Ahmed G, ym. Psychosocial Interventions for Attention Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis by the CADDRA Guidelines Work GROUP. Brain Sci 2022;12(8): «PMID: 36009086»PubMed
- Markel C. Child-focused psychosocial interventions for children and adolescents with attention-deficit hyperactivity disorder (ADHD): A systematic review and meta-analysis. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2018;78(8-B(E)):No-Specified
- Riise EN, Wergeland GJH, Njardvik U, ym. Cognitive behavior therapy for externalizing disorders in children and adolescents in routine clinical care: A systematic review and meta-analysis. Clin Psychol Rev 2021;83():101954 «PMID: 33418192»PubMed
- Anastopoulos AD. Facilitating parental understanding and management of attention-deficit/hyperactivity disorder. In: Reinecke MA DF, Freeman A (toim.), editor. Cognitive Therapy with Children and Adolescents. New York: The Guilford Press; 1996. p. 327-43
- Ranta K, Kauppi A. Lasten ja nuorten kognitiivinen psykoterapia. Kirjassa: Lastenpsykiatria ja Nuorisopsykiatria. Duodecim 2024:575-78
- Pettersson R, Söderström S, Edlund-Söderström K, ym. Internet-Based Cognitive Behavioral Therapy for Adults With ADHD in Outpatient Psychiatric Care. J Atten Disord 2017;21(6):508-521 «PMID: 24970720»PubMed
- Nasri B, Cassel M, Enhärje J, ym. Internet delivered cognitive behavioral therapy for adults with ADHD - A randomized controlled trial. Internet Interv 2023;33():100636 «PMID: 37483263»PubMed
- Novak I, Honan I. Effectiveness of paediatric occupational therapy for children with disabilities: A systematic review. Aust Occup Ther J 2019;66(3):258-273 «PMID: 30968419»PubMed
- Adamou M, Asherson P, Arif M, ym. Recommendations for occupational therapy interventions for adults with ADHD: a consensus statement from the UK adult ADHD network. BMC Psychiatry 2021;21(1):72 «PMID: 33541313»PubMed
- Nyfors H. Selvitys neuropsykiatrisen valmennuksen käytöstä ja koulutuksesta. Sosiaali- ja terveysministeriö. Raportteja ja muistioita 2022:20
- Catalá-López F, Hutton B, Núñez-Beltrán A, ym. The pharmacological and non-pharmacological treatment of attention deficit hyperactivity disorder in children and adolescents: A systematic review with network meta-analyses of randomised trials. PLoS One 2017;12(7):e0180355 «PMID: 28700715»PubMed
- Puustjärvi A, Putkonen H, Sumia M ym. ADHD:n lääkehoitoa ei tarvitse pelätä – vinkkejä käytännön työhön. Suom Lääkäril 2025, painossa
- Van Vyve L, Dierckx B, Lim CG, ym. Pharmacotherapy for ADHD in children and adolescents: A summary and overview of different European guidelines. Eur J Pediatr 2024;183(3):1047-1056 «PMID: 38095716»PubMed
- Cortese S, Adamo N, Del Giovane C, ym. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. Lancet Psychiatry 2018;5(9):727-738 «PMID: 30097390»PubMed
- O'Connor L, Carbone S, Gobbo A, ym. Pediatric attention deficit hyperactivity disorder (ADHD): 2022 updates on pharmacological management. Expert Rev Clin Pharmacol 2023;16(9):799-812 «PMID: 37587841»PubMed
- Kollins SH, Jain R, Brams M, ym. Clonidine extended-release tablets as add-on therapy to psychostimulants in children and adolescents with ADHD. Pediatrics 2011;127(6):e1406-13 «PMID: 21555501»PubMed
- Hammerness P, Georgiopoulos A, Doyle RL, ym. An open study of adjunct OROS-methylphenidate in children who are atomoxetine partial responders: II. Tolerability and pharmacokinetics. J Child Adolesc Psychopharmacol 2009;19(5):493-9 «PMID: 19877973»PubMed
- European Medicines Agency. Questions and answers on the review of medicines containing methylphenidate. London, 22 January 2009 Doc. Ref. EMEA/658285/2008
- Ornoy A, Koren G. The Effects of Drugs used for the Treatment of Attention Deficit Hyperactivity Disorder (ADHD) on Pregnancy Outcome and Breast-feeding: A Critical Review. Curr Neuropharmacol 2021;19(11):1794-1804 «PMID: 33245274»PubMed
- Scoten O, Tabi K, Paquette V, ym. Attention-deficit/hyperactivity disorder in pregnancy and the postpartum period. Am J Obstet Gynecol 2024;231(1):19-35 «PMID: 38432409»PubMed
- National Library of Medicine. Drugs and Lactation Database (LactMed®), https://www.ncbi.nlm.nih.gov/books/NBK501922/
- di Giacomo E, Confalonieri V, Tofani F, ym. Methylphenidate and Atomoxetine in Pregnancy and Possible Adverse Fetal Outcomes: A Systematic Review and Meta-Analysis. JAMA Netw Open 2024;7(11):e2443648 «PMID: 39504019»PubMed
- Bang Madsen K, Robakis TK, Liu X, ym. In utero exposure to ADHD medication and long-term offspring outcomes. Mol Psychiatry 2023;28(4):1739-1746 «PMID: 36759544»PubMed
- Korkeila J, Leppämäki S. ADHD. Kirjassa: Psykiatria. Kustannus Oy Duodecim 2014
- Stahl S. Stahl´s Essential Psychopharmacology. Neuroscientific Basis and Practical Applications. Fourth edition. Cambridge University Press.
- Coulter MK, Dean ME. Homeopathy for attention deficit/hyperactivity disorder or hyperkinetic disorder. Cochrane Database Syst Rev 2007;(4):CD005648 «PMID: 17943868»PubMed
- Rotella F, Cassioli E, Falone A, ym. Homeopathic Remedies in Psychiatric Disorders: A Meta-analysis of Randomized Controlled Trials. J Clin Psychopharmacol 2020;40(3):269-275 «PMID: 32332462»PubMed
- Panahandeh G, Vatani B, Safavi P, ym. The effect of adding ferrous sulfate to methylphenidate on attention-deficit/hyperactivity disorder in children. J Adv Pharm Technol Res 2017;8(4):138-142 «PMID: 29184845»PubMed
- Konofal E, Lecendreux M, Deron J, ym. Effects of iron supplementation on attention deficit hyperactivity disorder in children. Pediatr Neurol 2008;38(1):20-6 «PMID: 18054688»PubMed
- Granero R, Pardo-Garrido A, Carpio-Toro IL, ym. The Role of Iron and Zinc in the Treatment of ADHD among Children and Adolescents: A Systematic Review of Randomized Clinical Trials. Nutrients 2021;13(11): «PMID: 34836314»PubMed
- Ryhänen S, Vepsäläinen K, Huurre A, ym. Pienentynyt ferritiinipitoisuus lapsella: niukat rautavarastot ilman anemiaa. Suom lääkäril 2020;275:254-7
- Cortese S, Angriman M, Lecendreux M, ym. Iron and attention deficit/hyperactivity disorder: What is the empirical evidence so far? A systematic review of the literature. Expert Rev Neurother 2012;12(10):1227-40 «PMID: 23082739»PubMed
- Wang Y, Huang L, Zhang L, ym. Iron Status in Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis. PLoS One 2017;12(1):e0169145 «PMID: 28046016»PubMed
- Hariri M, Azadbakht L. Magnesium, Iron, and Zinc Supplementation for the Treatment of Attention Deficit Hyperactivity Disorder: A Systematic Review on the Recent Literature. Int J Prev Med 2015;6():83 «PMID: 26445630»PubMed
- Heilskov Rytter MJ, Andersen LB, Houmann T, ym. Diet in the treatment of ADHD in children - a systematic review of the literature. Nord J Psychiatry 2015;69(1):1-18 «PMID: 24934907»PubMed
- Uldall Torp NM, Thomsen PH. The use of diet interventions to treat symptoms of ADHD in children and adolescents - a systematic review of randomized controlled trials. Nord J Psychiatry 2020;74(8):558-568 «PMID: 32513046»PubMed
- Lange KW, Lange KM, Nakamura Y, ym. Nutrition in the Management of ADHD: A Review of Recent Research. Curr Nutr Rep 2023;12(3):383-394 «PMID: 37505402»PubMed
- Shareghfarid E, Sangsefidi ZS, Salehi-Abargouei A, ym. Empirically derived dietary patterns and food groups intake in relation with Attention Deficit/Hyperactivity Disorder (ADHD): A systematic review and meta-analysis. Clin Nutr ESPEN 2020;36():28-35 «PMID: 32220366»PubMed
- Tung I, Li JJ, Meza JI, ym. Patterns of Comorbidity Among Girls With ADHD: A Meta-analysis. Pediatrics 2016;138(4): «PMID: 27694280»PubMed
- Zeanah CH, Chesher T, Boris NW, ym. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Reactive Attachment Disorder and Disinhibited Social Engagement Disorder. J Am Acad Child Adolesc Psychiatry 2016;55(11):990-1003 «PMID: 27806867»PubMed
- Kirby A, Salmon G, Edward L. Should Children with ADHD be Routinely Screened for Motor Coordination Problems? The role of the Paediatric Occupational Therapist. BJOT 2007;70:483-6
- Raynolds F. Occupational Therapy for Children with Attention Deficit Hyperactivity Disorder (ADHD), Part 2: a Multicentre Evaluation of an Assessment and Treatment Package. Therapy 2007;70: 439-48
- Kaiser ML, Schoemaker MM, Albaret JM, ym. What is the evidence of impaired motor skills and motor control among children with attention deficit hyperactivity disorder (ADHD)? Systematic review of the literature. Res Dev Disabil 2015;36C():338-357 «PMID: 25462494»PubMed
- Goulardins JB, Rigoli D, Licari M, ym. Attention deficit hyperactivity disorder and developmental coordination disorder: Two separate disorders or do they share a common etiology. Behav Brain Res 2015;292():484-92 «PMID: 26168770»PubMed
- Dellapiazza F, Michelon C, Vernhet C, ym. Sensory processing related to attention in children with ASD, ADHD, or typical development: results from the ELENA cohort. Eur Child Adolesc Psychiatry 2021;30(2):283-291 «PMID: 32215734»PubMed
- Stray LL, Kristensen Ø, Lomeland M, ym. Motor regulation problems and pain in adults diagnosed with ADHD. Behav Brain Funct 2013;9():18 «PMID: 23642255»PubMed
- Kamath MS, Dahm CR, Tucker JR, ym. Sensory profiles in adults with and without ADHD. Res Dev Disabil 2020;104():103696 «PMID: 32526674»PubMed
- Adra N, Cao A, Makris N, ym. Sensory Modulation Disorder and its Neural Circuitry in Adults with ADHD: A Pilot Study. Brain Imaging Behav 2021;15(2):930-940 «PMID: 32770315»PubMed
- Hyde C, Fuelscher I, Efron D, ym. Adolescents with ADHD and co-occurring motor difficulties show a distinct pattern of maturation within the corticospinal tract from those without: A longitudinal fixel-based study. Hum Brain Mapp 2023;44(16):5504-5513 «PMID: 37608610»PubMed
- Mueller KL, Tomblin JB. Examining the comorbidity of language disorders and ADHD. Top Lang Disord 2012;32(3):228-246 «PMID: 25505812»PubMed
- Sciberras E, Mueller KL, Efron D, ym. Language problems in children with ADHD: a community-based study. Pediatrics 2014;133(5):793-800 «PMID: 24753530»PubMed
- Carruthers S, Taylor L, Sadiq H, ym. The profile of pragmatic language impairments in children with ADHD: A systematic review. Dev Psychopathol 2022;34(5):1938-1960 «PMID: 33973504»PubMed
- Korrel H, Mueller KL, Silk T, ym. Research Review: Language problems in children with Attention-Deficit Hyperactivity Disorder - a systematic meta-analytic review. J Child Psychol Psychiatry 2017;58(6):640-654 «PMID: 28186338»PubMed
- Méndez-Freije I, Areces D, Rodríguez C. Language Skills in Children with Attention Deficit Hyperactivity Disorder and Developmental Language Disorder: A Systematic Review. Children (Basel) 2023;11(1): «PMID: 38275435»PubMed
- Parks KMA, Hannah KE, Moreau CN, ym. Language abilities in children and adolescents with DLD and ADHD: A scoping review. J Commun Disord 2023;106():106381 «PMID: 37797400»PubMed
- Frazier TW, Youngstrom EA, Glutting JJ, ym. ADHD and achievement: meta-analysis of the child, adolescent, and adult literatures and a concomitant study with college students. J Learn Disabil 2007;40(1):49-65 «PMID: 17274547»PubMed
- Sexton CC, Gelhorn HL, Bell JA, ym. The co-occurrence of reading disorder and ADHD: epidemiology, treatment, psychosocial impact, and economic burden. J Learn Disabil 2012;45(6):538-64 «PMID: 21757683»PubMed
- DuPaul GJ, Gormley MJ, Laracy SD. Comorbidity of LD and ADHD: implications of DSM-5 for assessment and treatment. J Learn Disabil 2013;46(1):43-51 «PMID: 23144063»PubMed
- Barkley R, Murphy KR, Fischer M. ADHD in adults: what the science says. New York: The Guilford Press 2008
- Tervo T, Michelsson K, Launes J, ym. A Prospective 30-Year Follow-Up of ADHD Associated With Perinatal Risks. J Atten Disord 2017;21(10):799-810 «PMID: 25163542»PubMed
- Taanila A, Ebeling H, Tiihala M, ym. Association between childhood specific learning difficulties and school performance in adolescents with and without ADHD symptoms: a 16-year follow-up. J Atten Disord 2014;18(1):61-72 «PMID: 22751677»PubMed
- Leyfer OT, Folstein SE, Bacalman S, ym. Comorbid psychiatric disorders in children with autism: interview development and rates of disorders. J Autism Dev Disord 2006;36(7):849-61 «PMID: 16845581»PubMed
- Rommelse NN, Franke B, Geurts HM, ym. Shared heritability of attention-deficit/hyperactivity disorder and autism spectrum disorder. Eur Child Adolesc Psychiatry 2010;19(3):281-95 «PMID: 20148275»PubMed
- Supekar K, Iyer T, Menon V. The influence of sex and age on prevalence rates of comorbid conditions in autism. Autism Res 2017;10(5):778-789 «PMID: 28188687»PubMed
- Hartman CA, Geurts HM, Franke B, ym. Changing ASD-ADHD symptom co-occurrence across the lifespan with adolescence as crucial time window: Illustrating the need to go beyond childhood. Neurosci Biobehav Rev 2016;71():529-541 «PMID: 27629802»PubMed
- Ji N, Findling RL. An update on pharmacotherapy for autism spectrum disorder in children and adolescents. Curr Opin Psychiatry 2015;28(2):91-101 «PMID: 25602248»PubMed
- Beherec L, Quilici G, Rosier A, Gerardin P, Campion D, Guillin O. [Pharmacological treatments in patients with pervasive developmental disorders: A review]. Encephale 2014;40:188-96
- Baribeau DA, Anagnostou E. An update on medication management of behavioral disorders in autism. Curr Psychiatry Rep 2014;16(3):437 «PMID: 24488702»PubMed
- Reichow B, Volkmar FR, Bloch MH. Systematic review and meta-analysis of pharmacological treatment of the symptoms of attention-deficit/hyperactivity disorder in children with pervasive developmental disorders. J Autism Dev Disord 2013;43(10):2435-41 «PMID: 23468071»PubMed
- Scahill L, McCracken JT, King BH, ym. Extended-Release Guanfacine for Hyperactivity in Children With Autism Spectrum Disorder. Am J Psychiatry 2015;172(12):1197-206 «PMID: 26315981»PubMed
- Mahajan R, Bernal MP, Panzer R, ym. Clinical practice pathways for evaluation and medication choice for attention-deficit/hyperactivity disorder symptoms in autism spectrum disorders. Pediatrics 2012;130 Suppl 2():S125-38 «PMID: 23118243»PubMed
- Hirschtritt ME, Lee PC, Pauls DL, ym. Lifetime prevalence, age of risk, and genetic relationships of comorbid psychiatric disorders in Tourette syndrome. JAMA Psychiatry 2015;72(4):325-33 «PMID: 25671412»PubMed
- Puustjärvi A, Raaska H. Tourette oireyhtymä ja muut tic-häiriöt. Kirjassa Lastenpsykiatria ja nuorisopsykiatria. Kustannus Oy Duodecim 2025, sivut 313-320
- Andrén P, Jakubovski E, Murphy TL, ym. European clinical guidelines for Tourette syndrome and other tic disorders-version 2.0. Part II: psychological interventions. Eur Child Adolesc Psychiatry 2022;31(3):403-423 «PMID: 34313861»PubMed
- Johnson KA, Worbe Y, Foote KD, ym. Tourette syndrome: clinical features, pathophysiology, and treatment. Lancet Neurol 2023;22(2):147-158 «PMID: 36354027»PubMed
- Roessner V, Eichele H, Stern JS, ym. European clinical guidelines for Tourette syndrome and other tic disorders-version 2.0. Part III: pharmacological treatment. Eur Child Adolesc Psychiatry 2022;31(3):425-441 «PMID: 34757514»PubMed
- Osland ST, Steeves TD, Pringsheim T. Pharmacological treatment for attention deficit hyperactivity disorder (ADHD) in children with comorbid tic disorders. Cochrane Database Syst Rev 2018;6(6):CD007990 «PMID: 29944175»PubMed
- Cortese S, Faraone SV, Konofal E, ym. Sleep in children with attention-deficit/hyperactivity disorder: meta-analysis of subjective and objective studies. J Am Acad Child Adolesc Psychiatry 2009;48(9):894-908 «PMID: 19625983»PubMed
- Bondopadhyay U, Diaz-Orueta U, Coogan AN. A Systematic Review of Sleep and Circadian Rhythms in Children with Attention Deficit Hyperactivity Disorder. J Atten Disord 2022;26(2):149-224 «PMID: 33402013»PubMed
- Martins R, Scalco JC, Ferrari Junior GJ, ym. Sleep disturbance in children with attention-deficit hyperactivity disorder: A systematic review. Sleep Sci 2019;12(4):295-301 «PMID: 32318251»PubMed
- Arias-Mera C, Paillama-Raimán D, Lucero-González N, ym. Relation between sleep disorders and attention deficit disorder with hyperactivity in children and adolescents: A systematic review. Res Dev Disabil 2023;137():104500 «PMID: 37075589»PubMed
- Unettomuus. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Unitutkimusseura ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2023 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi.
- Sobanski E, Schredl M, Kettler N, ym. Sleep in adults with attention deficit hyperactivity disorder (ADHD) before and during treatment with methylphenidate: a controlled polysomnographic study. Sleep 2008;31(3):375-81 «PMID: 18363314»PubMed
- Paavonen J, Sarvasmaa AS. Unihäiriöt. Kirjassa: Lastenpsykiatria ja nuorisopsykiatria. Kustannus Oy Duodecim 2025, sivut 442-463
- Larsson I, Aili K, Lönn M, ym. Sleep interventions for children with attention deficit hyperactivity disorder (ADHD): A systematic literature review. Sleep Med 2023;102():64-75 «PMID: 36603513»PubMed
- Malkani MK, Pestell CF, Sheridan AMC, ym. Behavioral Sleep Interventions for Children With ADHD: A Systematic Review and Meta-Analysis. J Atten Disord 2022;26(14):1805-1821 «PMID: 35758199»PubMed
- Weiss MD, Wasdell MB, Bomben MM, ym. Sleep hygiene and melatonin treatment for children and adolescents with ADHD and initial insomnia. J Am Acad Child Adolesc Psychiatry 2006;45(5):512-519 «PMID: 16670647»PubMed
- Van der Heijden KB, Smits MG, Van Someren EJ, ym. Effect of melatonin on sleep, behavior, and cognition in ADHD and chronic sleep-onset insomnia. J Am Acad Child Adolesc Psychiatry 2007;46(2):233-41 «PMID: 17242627»PubMed
- Coogan AN, McGowan NM. A systematic review of circadian function, chronotype and chronotherapy in attention deficit hyperactivity disorder. Atten Defic Hyperact Disord 2017;9(3):129-147 «PMID: 28064405»PubMed
- Parvataneni T, Srinivas S, Shah K, ym. Perspective on Melatonin Use for Sleep Problems in Autism and Attention-Deficit Hyperactivity Disorder: A Systematic Review of Randomized Clinical Trials. Cureus 2020;12(5):e8335 «PMID: 32617211»PubMed
- Wang S, Yao B, Zhang H, ym. Comorbidity of epilepsy and attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. J Neurol 2023;270(9):4201-4213 «PMID: 37326829»PubMed
- Ono KE, Bearden DJ, Lee SM, ym. Interventions for ADHD in children & adolescents with epilepsy: A review and decision tree to guide clinicians. Epilepsy Behav 2022;135():108872 «PMID: 36037580»PubMed
- Rheims S, Auvin S. Attention deficit/hyperactivity disorder and epilepsy. Curr Opin Neurol 2021;34(2):219-225 «PMID: 33464761»PubMed
- Fan HC, Chiang KL, Chang KH, ym. Epilepsy and Attention Deficit Hyperactivity Disorder: Connection, Chance, and Challenges. Int J Mol Sci 2023;24(6): «PMID: 36982345»PubMed
- Reilly CJ. Attention deficit hyperactivity disorder (ADHD) in childhood epilepsy. Res Dev Disabil 2011;32(3):883-93 «PMID: 21310586»PubMed
- Brikell I, Chen Q, Kuja-Halkola R, ym. Medication treatment for attention-deficit/hyperactivity disorder and the risk of acute seizures in individuals with epilepsy. Epilepsia 2019;60(2):284-293 «PMID: 30682219»PubMed
- Wiggs KK, Chang Z, Quinn PD, ym. Attention-deficit/hyperactivity disorder medication and seizures. Neurology 2018;90(13):e1104-e1110 «PMID: 29476037»PubMed
- Antshel KM, Phillips MH, Gordon M, ym. Is ADHD a valid disorder in children with intellectual delays? Clin Psychol Rev 2006;26(5):555-72 «PMID: 16687197»PubMed
- Deutsch CK, Dube WV, McIlvane WJ. Attention deficits, Attention-Deficit Hyperactivity Disorder, and intellectual disabilities. Dev Disabil Res Rev 2008;14(4):285-92 «PMID: 19072752»PubMed
- Li Q, Li Y, Zheng J, ym. Prevalence and trends of developmental disabilities among US children and adolescents aged 3 to 17 years, 2018-2021. Sci Rep 2023;13(1):17254 «PMID: 37828147»PubMed
- Perera B, Chen J, Korb L, ym. Patterns of comorbidity and psychopharmacology in adults with intellectual disability and attention deficit hyperactivity disorder: an UK national cross-sectional audit. Expert Opin Pharmacother 2021;22(8):1071-1078 «PMID: 33487043»PubMed
- Freeman NC, Gray KM, Taffe JR, ym. Development of a New Attention Rating Scale for Children With Intellectual Disability: The Scale of Attention in Intellectual Disability (SAID). Am J Intellect Dev Disabil 2015;120(2):91-109 «PMID: 25715180»PubMed
- Freeman NC, Gray KM, Taffe JR, ym. A cross-syndrome evaluation of a new attention rating scale: The Scale of Attention in Intellectual Disability. Res Dev Disabil 2016;57():18-28 «PMID: 27348856»PubMed
- Perera B, Courtenay K, Solomou S, ym. Diagnosis of Attention Deficit Hyperactivity Disorder in Intellectual Disability: Diagnostic and Statistical Manual of Mental Disorder V versus clinical impression. J Intellect Disabil Res 2020;64(3):251-257 «PMID: 31808234»PubMed
- Arias VB, Arias B, Burns GL, ym. Invariance of parent ratings of attention deficit hyperactivity disorder symptoms for children with and without intellectual disability. J Appl Res Intellect Disabil 2019;32(2):288-299 «PMID: 30156358»PubMed
- Sun CK, Tseng PT, Wu CK, ym. Therapeutic effects of methylphenidate for attention-deficit/hyperactivity disorder in children with borderline intellectual functioning or intellectual disability: A systematic review and meta-analysis. Sci Rep 2019;9(1):15908 «PMID: 31685858»PubMed
- Tarrant N, Roy M, Deb S, ym. The effectiveness of methylphenidate in the management of Attention Deficit Hyperactivity Disorder (ADHD) in people with intellectual disabilities: A systematic review. Res Dev Disabil 2018;83():217-232 «PMID: 30266025»PubMed
- Tesli N, Jaholkowski P, Haukvik UK, ym. Conduct disorder - a comprehensive exploration of comorbidity patterns, genetic and environmental risk factors. Psychiatry Res 2024;331():115628 «PMID: 38029627»PubMed
- Connor DF, Steeber J, McBurnett K. A review of attention-deficit/hyperactivity disorder complicated by symptoms of oppositional defiant disorder or conduct disorder. J Dev Behav Pediatr 2010;31(5):427-40 «PMID: 20535081»PubMed
- Caye A, Spadini AV, Karam RG, ym. Predictors of persistence of ADHD into adulthood: a systematic review of the literature and meta-analysis. Eur Child Adolesc Psychiatry 2016;25(11):1151-1159 «PMID: 27021056»PubMed
- Gurnani T, Ivanov I, Newcorn JH. Pharmacotherapy of Aggression in Child and Adolescent Psychiatric Disorders. J Child Adolesc Psychopharmacol 2016;26(1):65-73 «PMID: 26881859»PubMed
- Aronen E, Takala L, Haravuori H. Traumaperäiset stressihäiriöt ja sopeutumishäiriöt. Kirjassa: Lastenpsykiatria ja nuorisopsykiatria. Duodecim 2024:370-380
- Koenen KC, Moffitt TE, Poulton R, ym. Early childhood factors associated with the development of post-traumatic stress disorder: results from a longitudinal birth cohort. Psychol Med 2007;37(2):181-92 «PMID: 17052377»PubMed
- Spencer AE, Faraone SV, Bogucki OE, ym. Examining the association between posttraumatic stress disorder and attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. J Clin Psychiatry 2016;77(1):72-83 «PMID: 26114394»PubMed
- Antshel KM, Kaul P, Biederman J, ym. Posttraumatic stress disorder in adult attention-deficit/hyperactivity disorder: clinical features and familial transmission. J Clin Psychiatry 2013;74(3):e197-204 «PMID: 23561240»PubMed
- Harrington KM, Miller MW, Wolf EJ, ym. Attention-deficit/hyperactivity disorder comorbidity in a sample of veterans with posttraumatic stress disorder. Compr Psychiatry 2012;53(6):679-90 «PMID: 22305866»PubMed
- Martínez L, Prada E, Satler C, ym. Executive Dysfunctions: The Role in Attention Deficit Hyperactivity and Post-traumatic Stress Neuropsychiatric Disorders. Front Psychol 2016;7():1230 «PMID: 27602003»PubMed
- Zhang N, Gao M, Yu J, ym. Understanding the association between adverse childhood experiences and subsequent attention deficit hyperactivity disorder: A systematic review and meta-analysis of observational studies. Brain Behav 2022;12(10):e32748 «PMID: 36068993»PubMed
- Adler LA, Kunz M, Chua HC, ym. Attention-deficit/hyperactivity disorder in adult patients with posttraumatic stress disorder (PTSD): is ADHD a vulnerability factor? J Atten Disord 2004;8(1):11-6 «PMID: 15669598»PubMed
- Klein B, Damiani-Taraba G, Koster A, ym. Diagnosing attention-deficit hyperactivity disorder (ADHD) in children involved with child protection services: are current diagnostic guidelines acceptable for vulnerable populations? Child Care Health Dev 2015;41(2):178-85 «PMID: 24942100»PubMed
- Daud A, Rydelius PA. Comorbidity/overlapping between ADHD and PTSD in relation to IQ among children of traumatized/non-traumatized parents. J Atten Disord 2009;13(2):188-96 «PMID: 19395643»PubMed
- Weinstein D, Staffelbach D, Biaggio M. Attention-deficit hyperactivity disorder and posttraumatic stress disorder: differential diagnosis in childhood sexual abuse. Clin Psychol Rev 2000;20(3):359-78 «PMID: 10779899»PubMed
- Blackmore R, Gray KM, Boyle JA, ym. Systematic Review and Meta-analysis: The Prevalence of Mental Illness in Child and Adolescent Refugees and Asylum Seekers. J Am Acad Child Adolesc Psychiatry 2020;59(6):705-714 «PMID: 31778780»PubMed
- Belkin MR, Schwartz TL. Alpha-2 receptor agonists for the treatment of posttraumatic stress disorder. Drugs Context 2015;4():212286 «PMID: 26322115»PubMed
- Lee DJ, Schnitzlein CW, Wolf JP, ym. PSYCHOTHERAPY VERSUS PHARMACOTHERAPY FOR POSTTRAUMATIC STRESS DISORDER: SYSTEMIC REVIEW AND META-ANALYSES TO DETERMINE FIRST-LINE TREATMENTS. Depress Anxiety 2016;33(9):792-806 «PMID: 27126398»PubMed
- Jagtiani A, Gandhi R, Banga A, ym. Alpha-2 Agonists in Children and Adolescents With Post-traumatic Stress Disorder: A Systematic Review. Cureus 2024;16(1):e53009 «PMID: 38410304»PubMed
- Njardvik U, Wergeland GJ, Riise EN, ym. Psychiatric comorbidity in children and adolescents with ADHD: A systematic review and meta-analysis. Clin Psychol Rev 2025;118():102571 «PMID: 40245462»PubMed
- Angold A, Costello EJ, Erkanli A. Comorbidity. J Child Psychol Psychiatry 1999;40(1):57-87 «PMID: 10102726»PubMed
- Steinhausen HC, Nøvik TS, Baldursson G, ym. Co-existing psychiatric problems in ADHD in the ADORE cohort. Eur Child Adolesc Psychiatry 2006;15 Suppl 1():I25-9 «PMID: 17177012»PubMed
- Ranta K, Koskinen M. Ahdistuneisuushäiriöt. Kirjassa: Lastenpsykiatria ja nuorisopsykiatria. Kustannus Oy Duodecim 2025, sivut 287-305
- Jakobsson Støre S, Van Zalk N, Granander Schwartz W, ym. The Relationship Between Social Anxiety Disorder and ADHD in Adolescents and Adults: A Systematic Review. J Atten Disord 2024;28(9):1299-1319 «PMID: 38651640»PubMed
- Schatz DB, Rostain AL. ADHD with comorbid anxiety: a review of the current literature. J Atten Disord 2006;10(2):141-9 «PMID: 17085624»PubMed
- Manassis K. When attention-deficit/hyperactivity disorder co-occurs with anxiety disorders: effects on treatment. Expert Rev Neurother 2007;7(8):981-8 «PMID: 17678493»PubMed
- León-Barriera R, Ortegon RS, Chaplin MM, ym. Treating ADHD and Comorbid Anxiety in Children: A Guide for Clinical Practice. Clin Pediatr (Phila) 2023;62(1):39-46 «PMID: 35854648»PubMed
- Bryant A, Schlesinger H, Sideri A, ym. A meta-analytic review of the impact of ADHD medications on anxiety and depression in children and adolescents. Eur Child Adolesc Psychiatry 2023;32(10):1885-1898 «PMID: 35616714»PubMed
- Yao S, Kuja-Halkola R, Martin J, ym. Associations Between Attention-Deficit/Hyperactivity Disorder and Various Eating Disorders: A Swedish Nationwide Population Study Using Multiple Genetically Informative Approaches. Biol Psychiatry 2019;86(8):577-586 «PMID: 31301758»PubMed
- Villa FM, Crippa A, Rosi E, ym. ADHD and eating disorders in childhood and adolescence: An updated minireview. J Affect Disord 2023;321():265-271 «PMID: 36356347»PubMed
- Waring ME, Lapane KL. Overweight in children and adolescents in relation to attention-deficit/hyperactivity disorder: results from a national sample. Pediatrics 2008;122(1):e1-6 «PMID: 18595954»PubMed
- Mikami AY, Hinshaw SP, Arnold LE, ym. Bulimia nervosa symptoms in the multimodal treatment study of children with ADHD. Int J Eat Disord 2010;43(3):248-59 «PMID: 19378318»PubMed
- Cortese S, Isnard P, Frelut ML, ym. Association between symptoms of attention-deficit/hyperactivity disorder and bulimic behaviors in a clinical sample of severely obese adolescents. Int J Obes (Lond) 2007;31(2):340-6 «PMID: 16733525»PubMed
- Lihavuus (lapset, nuoret ja aikuiset). Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin, Suomen Lihavuustutkijat ry:n ja Suomen Lastenlääkäriyhdistys ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi.
- Syömishäiriöt. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin, Suomen Lastenpsykiatriyhdistys ry:n, Suomen Nuorisopsykiatrinen yhdistys ry:n ja Suomen Psykiatriyhdistys ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi.
- Michielsen M, Comijs HC, Semeijn EJ, ym. The comorbidity of anxiety and depressive symptoms in older adults with attention-deficit/hyperactivity disorder: a longitudinal study. J Affect Disord 2013;148(2-3):220-7 «PMID: 23267726»PubMed
- Meinzer MC, Pettit JW, Viswesvaran C. The co-occurrence of attention-deficit/hyperactivity disorder and unipolar depression in children and adolescents: a meta-analytic review. Clin Psychol Rev 2014;34(8):595-607 «PMID: 25455624»PubMed
- Meinzer MC, Lewinsohn PM, Pettit JW, ym. Attention-deficit/hyperactivity disorder in adolescence predicts onset of major depressive disorder through early adulthood. Depress Anxiety 2013;30(6):546-53 «PMID: 23424020»PubMed
- Powell V, Agha SS, Jones RB, ym. ADHD in adults with recurrent depression. J Affect Disord 2021;295():1153-1160 «PMID: 34706428»PubMed
- Thapar A, Livingston LA, Eyre O, ym. Practitioner Review: Attention-deficit hyperactivity disorder and autism spectrum disorder - the importance of depression. J Child Psychol Psychiatry 2023;64(1):4-15 «PMID: 35972029»PubMed
- Riglin L, Leppert B, Dardani C, ym. ADHD and depression: investigating a causal explanation. Psychol Med 2021;51(11):1890-1897 «PMID: 32249726»PubMed
- Remschmidt H, Global ADHD Working Group. Global consensus on ADHD/HKD. Eur Child Adolesc Psychiatry 2005;14(3):127-37 «PMID: 15959658»PubMed
- Guo C, Assumpcao L, Hu Z. Efficacy of Non-pharmacological Treatments on Emotional Symptoms of Children and Adults with Attention-Deficit/Hyperactivity Disorder: A Meta-Analysis. J Atten Disord 2022;26(4):508-524 «PMID: 33759605»PubMed
- Ljung T, Chen Q, Lichtenstein P, ym. Common etiological factors of attention-deficit/hyperactivity disorder and suicidal behavior: a population-based study in Sweden. JAMA Psychiatry 2014;71(8):958-64 «PMID: 24964928»PubMed
- Pozzi M, Carnovale C, Mazhar F, ym. Adverse Drug Reactions Related to Mood and Emotion in Pediatric Patients Treated for Attention Deficit/Hyperactivity Disorder: A Comparative Analysis of the US Food and Drug Administration Adverse Event Reporting System Database. J Clin Psychopharmacol 2019;39(4):386-392 «PMID: 31205193»PubMed
- Lee MJ, Yang KC, Shyu YC, ym. Attention-deficit hyperactivity disorder, its treatment with medication and the probability of developing a depressive disorder: A nationwide population-based study in Taiwan. J Affect Disord 2016;189():110-7 «PMID: 26433758»PubMed
- Krinzinger H, Hall CL, Groom MJ, ym. Neurological and psychiatric adverse effects of long-term methylphenidate treatment in ADHD: A map of the current evidence. Neurosci Biobehav Rev 2019;107():945-968 «PMID: 31545988»PubMed
- Frías Á, Palma C, Farriols N. Comorbidity in pediatric bipolar disorder: prevalence, clinical impact, etiology and treatment. J Affect Disord 2015;174():378-89 «PMID: 25545605»PubMed
- Sadeghian Nadooshan MR, Shahrivar Z, Mahmoudi Gharaie J, ym. ADHD in adults with major depressive or bipolar disorder: does it affect clinical features, comorbidity, quality of life, and global functioning? BMC Psychiatry 2022;22(1):707 «PMID: 36380307»PubMed
- Solberg BS, Halmøy A, Engeland A, ym. Gender differences in psychiatric comorbidity: a population-based study of 40 000 adults with attention deficit hyperactivity disorder. Acta Psychiatr Scand 2018;137(3):176-186 «PMID: 29266167»PubMed
- Merikangas KR, Jin R, He JP, ym. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry 2011;68(3):241-51 «PMID: 21383262»PubMed
- Schiweck C, Arteaga-Henriquez G, Aichholzer M, ym. Comorbidity of ADHD and adult bipolar disorder: A systematic review and meta-analysis. Neurosci Biobehav Rev 2021;124():100-123 «PMID: 33515607»PubMed
- Miskowiak KW, Obel ZK, Guglielmo R, ym. Efficacy and safety of established and off-label ADHD drug therapies for cognitive impairment or attention-deficit hyperactivity disorder symptoms in bipolar disorder: A systematic review by the ISBD Targeting Cognition Task Force. Bipolar Disord 2024;26(3):216-239 «PMID: 38433530»PubMed
- Pinna M, Visioli C, Rago CM, ym. Attention deficit-hyperactivity disorder in adult bipolar disorder patients. J Affect Disord 2019;243():391-396 «PMID: 30267955»PubMed
- Salvi V, Ribuoli E, Servasi M, ym. ADHD and Bipolar Disorder in Adulthood: Clinical and Treatment Implications. Medicina (Kaunas) 2021;57(5): «PMID: 34068605»PubMed
- Stutzman DL, Dopheide JA. Practice Pearls for Stimulant Treatment of Attention-Deficit/Hyperactivity Disorder in Youth. J Pediatr Pharmacol Ther 2024;29(3):215-231 «PMID: 38863854»PubMed
- van Hulzen KJE, Scholz CJ, Franke B, ym. Genetic Overlap Between Attention-Deficit/Hyperactivity Disorder and Bipolar Disorder: Evidence From Genome-wide Association Study Meta-analysis. Biol Psychiatry 2017;82(9):634-641 «PMID: 27890468»PubMed
- Als TD, Kurki MI, Grove J, ym. Depression pathophysiology, risk prediction of recurrence and comorbid psychiatric disorders using genome-wide analyses. Nat Med 2023;29(7):1832-1844 «PMID: 37464041»PubMed
- Khoury E, Acquaviva E, Purper-Ouakil D, ym. Meta-analysis of personal and familial co-occurrence of Attention Deficit/Hyperactivity Disorder and Bipolar Disorder. Neurosci Biobehav Rev 2023;146():105050 «PMID: 36657649»PubMed
- Hosang GM, Lichtenstein P, Ronald A, ym. Association of Genetic and Environmental Risks for Attention-Deficit/Hyperactivity Disorder With Hypomanic Symptoms in Youths. JAMA Psychiatry 2019;76(11):1150-1158 «PMID: 31411648»PubMed
- Goldstein BI, Birmaher B, Carlson GA, ym. The International Society for Bipolar Disorders Task Force report on pediatric bipolar disorder: Knowledge to date and directions for future research. Bipolar Disord 2017;19(7):524-543 «PMID: 28944987»PubMed
- Arnold LE, Van Meter AR, Fristad MA, ym. Development of bipolar disorder and other comorbidity among youth with attention-deficit/hyperactivity disorder. J Child Psychol Psychiatry 2020;61(2):175-181 «PMID: 31523819»PubMed
- Connors MH. Paediatric bipolar disorder and its controversy. Acta Neuropsychiatr 2023;35(2):96-103 «PMID: 36373500»PubMed
- Brickman HM, Fristad MA. Psychosocial Treatments for Bipolar Disorder in Children and Adolescents. Annu Rev Clin Psychol 2022;18():291-327 «PMID: 35216522»PubMed
- DelBello MP, Soutullo CA, Hendricks W, ym. Prior stimulant treatment in adolescents with bipolar disorder: association with age at onset. Bipolar Disord 2001;3(2):53-7 «PMID: 11333062»PubMed
- Jerrell JM, McIntyre RS, Park YM. Correlates of incident bipolar disorder in children and adolescents diagnosed with attention-deficit/hyperactivity disorder. J Clin Psychiatry 2014;75(11):e1278-83 «PMID: 25470092»PubMed
- Viktorin A, Rydén E, Thase ME, ym. The Risk of Treatment-Emergent Mania With Methylphenidate in Bipolar Disorder. Am J Psychiatry 2017;174(4):341-348 «PMID: 27690517»PubMed
- Tillman R, Geller B. Controlled study of switching from attention-deficit/hyperactivity disorder to a prepubertal and early adolescent bipolar I disorder phenotype during 6-year prospective follow-up: rate, risk, and predictors. Dev Psychopathol 2006;18(4):1037-53 «PMID: 17064428»PubMed
- Chiorean A, Jones BDM, Murong M, ym. Prescribed psychostimulants and other pro-cognitive medications in bipolar disorder: A systematic review and meta-analysis of recurrence of manic symptoms. Bipolar Disord 2024;26(5):418-430 «PMID: 38670627»PubMed
- O'Connor H, Hutt Vater C, DiSalvo M, ym. Stimulant Treatment and Potential Adverse Outcomes in Pediatric Populations With Bipolar Disorder: A Systematic Review of the Literature. J Atten Disord 2024;28(5):740-750 «PMID: 38156605»PubMed
- Wang LJ, Shyu YC, Yuan SS, ym. Attention-deficit hyperactivity disorder, its pharmacotherapy, and the risk of developing bipolar disorder: A nationwide population-based study in Taiwan. J Psychiatr Res 2016;72():6-14 «PMID: 26519764»PubMed
- Jefsen OH, Østergaard SD, Rohde C. Risk of Mania After Methylphenidate in Patients With Bipolar Disorder. J Clin Psychopharmacol 2023;43(1):28-34 «PMID: 36584246»PubMed
- Perugi G, Vannucchi G. The use of stimulants and atomoxetine in adults with comorbid ADHD and bipolar disorder. Expert Opin Pharmacother 2015;16(14):2193-204 «PMID: 26364896»PubMed
- Pataki C, Carlson GA. The comorbidity of ADHD and bipolar disorder: any less confusion? Curr Psychiatry Rep 2013;15(7):372 «PMID: 23712723»PubMed
- Scheffer RE, Kowatch RA, Carmody T, ym. Randomized, placebo-controlled trial of mixed amphetamine salts for symptoms of comorbid ADHD in pediatric bipolar disorder after mood stabilization with divalproex sodium. Am J Psychiatry 2005;162(1):58-64 «PMID: 15625202»PubMed
- Hah M, Chang K. Atomoxetine for the treatment of attention-deficit/hyperactivity disorder in children and adolescents with bipolar disorders. J Child Adolesc Psychopharmacol 2005;15(6):996-1004 «PMID: 16379520»PubMed
- Findling RL, Short EJ, McNamara NK, ym. Methylphenidate in the treatment of children and adolescents with bipolar disorder and attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 2007;46(11):1445-53 «PMID: 18049294»PubMed
- Chang K, Nayar D, Howe M, ym. Atomoxetine as an adjunct therapy in the treatment of co-morbid attention-deficit/hyperactivity disorder in children and adolescents with bipolar I or II disorder. J Child Adolesc Psychopharmacol 2009;19(5):547-51 «PMID: 19877979»PubMed
- Pouchon A, Nasserdine R, Dondé C, ym. A systematic review of pharmacotherapy for attention-deficit/hyperactivity disorder in children and adolescents with bipolar disorders. Expert Opin Pharmacother 2023;24(13):1497-1509 «PMID: 37300473»PubMed
- McIntyre RS, Alsuwaidan M, Soczynska JK, ym. The effect of lisdexamfetamine dimesylate on body weight, metabolic parameters, and attention deficit hyperactivity disorder symptomatology in adults with bipolar I/II disorder. Hum Psychopharmacol 2013;28(5):421-7 «PMID: 24014142»PubMed
- Dalsgaard S, Mortensen PB, Frydenberg M, ym. Association between Attention-Deficit Hyperactivity Disorder in childhood and schizophrenia later in adulthood. Eur Psychiatry 2014;29(4):259-63 «PMID: 24016863»PubMed
- Nourredine M, Gering A, Fourneret P, ym. Association of Attention-Deficit/Hyperactivity Disorder in Childhood and Adolescence With the Risk of Subsequent Psychotic Disorder: A Systematic Review and Meta-analysis. JAMA Psychiatry 2021;78(5):519-529 «PMID: 33625499»PubMed
- Toba-Oluboka T, Dempster K. A Narrative Review Exploring Attention Deficit/Hyperactivity Disorder in Patients with Early Psychosis. Brain Sci 2024;14(3): «PMID: 38539580»PubMed
- Hollis C, Chen Q, Chang Z, ym. Methylphenidate and the risk of psychosis in adolescents and young adults: a population-based cohort study. Lancet Psychiatry 2019;6(8):651-658 «PMID: 31221557»PubMed
- Mosholder AD, Gelperin K, Hammad TA, ym. Hallucinations and other psychotic symptoms associated with the use of attention-deficit/hyperactivity disorder drugs in children. Pediatrics 2009;123(2):611-6 «PMID: 19171629»PubMed
- Ross RG. Psychotic and manic-like symptoms during stimulant treatment of attention deficit hyperactivity disorder. Am J Psychiatry 2006;163(7):1149-52 «PMID: 16816217»PubMed
- Björkenstam E, Pierce M, Björkenstam C, ym. Attention Deficit/Hyperactivity Disorder and risk for non-affective psychotic disorder: The role of ADHD medication and comorbidity, and sibling comparison. Schizophr Res 2020;218():124-130 «PMID: 32001080»PubMed
- Shyu YC, Yuan SS, Lee SY, ym. Attention-deficit/hyperactivity disorder, methylphenidate use and the risk of developing schizophrenia spectrum disorders: A nationwide population-based study in Taiwan. Schizophr Res 2015;168(1-2):161-7 «PMID: 26363968»PubMed
- Moran LV, Skinner JP, Shinn AK, ym. Risk of Incident Psychosis and Mania With Prescription Amphetamines. Am J Psychiatry 2024;181(10):901-909 «PMID: 39262211»PubMed
- Bieś R, Fojcik J, Warchala A, ym. The Risk of Methylphenidate Pharmacotherapy for Adults with ADHD. Pharmaceuticals (Basel) 2023;16(9): «PMID: 37765100»PubMed
- Man KK, Coghill D, Chan EW, ym. Methylphenidate and the risk of psychotic disorders and hallucinations in children and adolescents in a large health system. Transl Psychiatry 2016;6(11):e956 «PMID: 27845780»PubMed
- Young S, Abbasian C, Al-Attar Z, ym. Identification and treatment of individuals with attention-deficit/hyperactivity disorder and substance use disorder: An expert consensus statement. World J Psychiatry 2023;13(3):84-112 «PMID: 37033892»PubMed
- Rohner H, Gaspar N, Philipsen A, ym. Prevalence of Attention Deficit Hyperactivity Disorder (ADHD) among Substance Use Disorder (SUD) Populations: Meta-Analysis. Int J Environ Res Public Health 2023;20(2): «PMID: 36674031»PubMed
- Molina BSG, Kennedy TM, Howard AL, ym. Association Between Stimulant Treatment and Substance Use Through Adolescence Into Early Adulthood. JAMA Psychiatry 2023;80(9):933-941 «PMID: 37405756»PubMed
- Crunelle CL, van den Brink W, Moggi F, ym. International Consensus Statement on Screening, Diagnosis and Treatment of Substance Use Disorder Patients with Comorbid Attention Deficit/Hyperactivity Disorder. Eur Addict Res 2018;24(1):43-51 «PMID: 29510390»PubMed
- van Amsterdam J, van der Velde B, Schulte M, ym. Causal Factors of Increased Smoking in ADHD: A Systematic Review. Subst Use Misuse 2018;53(3):432-445 «PMID: 29039714»PubMed
- Schoenfelder EN, Faraone SV, Kollins SH. Stimulant treatment of ADHD and cigarette smoking: a meta-analysis. Pediatrics 2014;133(6):1070-80 «PMID: 24819571»PubMed
- Carpentier PJ, Levin FR. Pharmacological Treatment of ADHD in Addicted Patients: What Does the Literature Tell Us? Harv Rev Psychiatry 2017;25(2):50-64 «PMID: 28272130»PubMed
- Zaso MJ, Park A, Antshel KM. Treatments for Adolescents With Comorbid ADHD and Substance Use Disorder: A Systematic Review. J Atten Disord 2020;24(9):1215-1226 «PMID: 25655767»PubMed
- Lee LC, Harrington RA, Chang JJ, ym. Increased risk of injury in children with developmental disabilities. Res Dev Disabil 2008;29(3):247-55 «PMID: 17582739»PubMed
- Palili A, Kolaitis G, Vassi I, ym. Inattention, hyperactivity, impulsivity--epidemiology and correlations: a nationwide greek study from birth to 18 years. J Child Neurol 2011;26(2):199-204 «PMID: 20921568»PubMed
- Garzon DL, Huang H, Todd RD. Do attention deficit/hyperactivity disorder and oppositional defiant disorder influence preschool unintentional injury risk? Arch Psychiatr Nurs 2008;22(5):288-96 «PMID: 18809121»PubMed
- Erskine HE, Norman RE, Ferrari AJ, ym. Long-Term Outcomes of Attention-Deficit/Hyperactivity Disorder and Conduct Disorder: A Systematic Review and Meta-Analysis. J Am Acad Child Adolesc Psychiatry 2016;55(10):841-50 «PMID: 27663939»PubMed
- Libutzki B, Neukirch B, Kittel-Schneider S, ym. Risk of accidents and unintentional injuries in men and women with attention deficit hyperactivity disorder across the adult lifespan. Acta Psychiatr Scand 2023;147(2):145-154 «PMID: 36464800»PubMed
- Schwebel DC, Speltz ML, Jones K, ym. Unintentional injury in preschool boys with and without early onset of disruptive behavior. J Pediatr Psychol 2002;27(8):727-37 «PMID: 12403863»PubMed
- Schwebel DC, Hodgens JB, Sterling S. How mothers parent their children with behavior disorders: implications for unintentional injury risk. J Safety Res 2006;37(2):167-73 «PMID: 16674977»PubMed
- So M, Dziuban EJ, Pedati CS, ym. Childhood Physical Health and Attention Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis of Modifiable Factors. Prev Sci 2024;25(Suppl 2):316-336 «PMID: 35947281»PubMed
- Fischer M, Barkley RA, Smallish L, ym. Hyperactive children as young adults: driving abilities, safe driving behavior, and adverse driving outcomes. Accid Anal Prev 2007;39(1):94-105 «PMID: 16919226»PubMed
- Brunkhorst-Kanaan N, Libutzki B, Reif A, ym. ADHD and accidents over the life span - A systematic review. Neurosci Biobehav Rev 2021;125():582-591 «PMID: 33582234»PubMed
- Ruiz-Goikoetxea M, Cortese S, Aznarez-Sanado M, ym. Risk of unintentional injuries in children and adolescents with ADHD and the impact of ADHD medications: A systematic review and meta-analysis. Neurosci Biobehav Rev 2018;84():63-71 «PMID: 29162520»PubMed
- Vasiliadis HM, Lunghi C, Rahme E, ym. ADHD medications use and risk of mortality and unintentional injuries: a population-based cohort study. Transl Psychiatry 2024;14(1):128 «PMID: 38418443»PubMed
- Carr RH, Eom GD, Brown EE. Attention-Deficit/Hyperactivity Disorder as a Potential Risk Factor for Dementia and Other Neurocognitive Disorders: A Systematic Review. J Alzheimers Dis 2024;98(3):773-792 «PMID: 38461502»PubMed
- Becker S, Chowdhury M, Tavilsup P, ym. Risk of neurodegenerative disease or dementia in adults with attention-deficit/hyperactivity disorder: a systematic review. Front Psychiatry 2023;14():1158546 «PMID: 37663597»PubMed
- Stein DS, Blum NJ, Barbaresi WJ. Developmental and behavioral disorders through the life span. Pediatrics 2011;128(2):364-73 «PMID: 21768324»PubMed
- Mordre M, Groholt B, Sandstad B, ym. The impact of ADHD symptoms and global impairment in childhood on working disability in mid-adulthood: a 28-year follow-up study using official disability pension records in a high-risk in-patient population. BMC Psychiatry 2012;12():174 «PMID: 23083209»PubMed
- Nordby ES, Guribye F, Nordgreen T, ym. Silver linings of ADHD: a thematic analysis of adults' positive experiences with living with ADHD. BMJ Open 2023;13(10):e072052 «PMID: 37788928»PubMed
- Huang W, Yuan C, Li M. Person-Job Fit and Innovation Behavior: Roles of Job Involvement and Career Commitment. Front Psychol 2019;10():1134 «PMID: 31156521»PubMed
- Vaaramo M. Studies on occupational choice, temperament traits, and economic preferences. Oulun yliopisto 05.12.2024. https://urn.fi/URN:NBN:fi:oulu-202411126721
- Seidman LJ, Biederman J, Weber W, ym. Neuropsychological function in adults with attention-deficit hyperactivity disorder. Biol Psychiatry 1998;44(4):260-8 «PMID: 9715357»PubMed
- Chang Z, Lichtenstein P, D'Onofrio BM, ym. Serious transport accidents in adults with attention-deficit/hyperactivity disorder and the effect of medication: a population-based study. JAMA Psychiatry 2014;71(3):319-25 «PMID: 24477798»PubMed
- Halt AH, Uusitalo J, Niemi P, ym. Military performance of men with attention-deficit/hyperactivity disorder: findings from a follow-up study in the Northern Finland birth cohort 1986. Nord J Psychiatry 2023;77(1):96-101 «PMID: 36309808»PubMed
- Rautanen M, Harald K, Tyni S. Vankien terveys ja hyvinvointi 2023. Terveyden ja hyvinvoinnin laitos (THL). Raportti 007/2023. 256 sivua. Helsinki 2023. http://urn.fi/URN:ISBN:978-952-408-148-1
- Kriminalvården. 2021. Neuropsykiatrisk utredningsrutin och behandlingsrekommendationer v4, diarienummer 2015-027370
- Catalá-López F, Hutton B, Page MJ, ym. Mortality in Persons With Autism Spectrum Disorder or Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-analysis. JAMA Pediatr 2022;176(4):e216401 «PMID: 35157020»PubMed
- Sun S, Kuja-Halkola R, Faraone SV, ym. Association of Psychiatric Comorbidity With the Risk of Premature Death Among Children and Adults With Attention-Deficit/Hyperactivity Disorder. JAMA Psychiatry 2019;76(11):1141-1149 «PMID: 31389973»PubMed
- Li L, Zhu N, Zhang L, ym. ADHD Pharmacotherapy and Mortality in Individuals With ADHD. JAMA 2024;331(10):850-860 «PMID: 38470385»PubMed
- Danckaerts M, Sonuga-Barke EJ, Banaschewski T, ym. The quality of life of children with attention deficit/hyperactivity disorder: a systematic review. Eur Child Adolesc Psychiatry 2010;19(2):83-105 «PMID: 19633992»PubMed
- Mohr-Jensen C, Steinhausen HC. A meta-analysis and systematic review of the risks associated with childhood attention-deficit hyperactivity disorder on long-term outcome of arrests, convictions, and incarcerations. Clin Psychol Rev 2016;48():32-42 «PMID: 27390061»PubMed
- Connor DF, Carlson GA, Chang KD, ym. Juvenile maladaptive aggression: a review of prevention, treatment, and service configuration and a proposed research agenda. J Clin Psychiatry 2006;67(5):808-20 «PMID: 16841631»PubMed
- Prasad S, Harpin V, Poole L, ym. A multi-centre, randomised, open-label study of atomoxetine compared with standard current therapy in UK children and adolescents with attention-deficit/hyperactivity disorder (ADHD). Curr Med Res Opin 2007;23(2):379-94 «PMID: 17288692»PubMed