

Parodontiitti
Miten viitata Käypä hoito -suositukseen? «K1»1
Keskeinen sanoma
- Parodontiitti eli hampaan kiinnityskudossairaus on merkittävä kansantauti. Se on väestössä alidiagnosoitu ja jää sen takia usein hoitamatta. Sairauden merkkejä nähdään myös lapsilla ja nuorilla.
- Gingiviitin eli ientulehduksen ehkäisy ja hoito ovat keskeinen osa kiinnityskudosten terveydenhoitoa ja parodontiitin ehkäisyä. Erityisesti lasten ja nuorten gingiviitin ja parodontiitin ehkäisyssä keskeistä on ohjaus hyvien omahoitotapojen vakiinnuttamiseksi.
- Tupakka- sekä nikotiinituotteiden käytön ehkäisy on keskeistä parodontiitin ehkäisyssä.
- Parodontiitin diagnostiikkaan ja hoitoon on kohdistettava erityistä huomiota, sillä pitkälle edennyt parodontiitti vaatii usein erikoishammaslääkäritasoista hoitoa ja aiheuttaa huomattavia kustannuksia.
- Parodontiittiriskin toteaminen edistää ehkäisyn ja hoidon kohdentamista.
- Parodontologinen tutkimus, johon kuuluu olennaisesti ientaskumittaus, on osa suun terveydentilan tutkimusta ja sisältää myös peri-implanttikudosten tutkimisen. Tutkimus pitää tehdä kaikenikäisille säännöllisin väliajoin, jotta hampaita ja hammasimplantteja ympäröivien kudosten sairaudet todetaan varhaisessa vaiheessa.
- Hammaslääkäri vastaa diagnostiikasta, hoidon suunnittelusta ja hoidon toteutuksesta.
- Kun sairaus on diagnosoitu, se hoidetaan viipymättä. Vaikuttava hoito on toteutettavissa tehokkaasti lyhyellä aikavälillä.
- Tärkeä osa hoitoa ovat omahoidon ohjaus, potilaan sitouttaminen hoitoon sekä tupakka- ja nikotiinituotteiden käytön ehkäisy ja tarvittaessa tupakka- ja nikotiinituotteista vieroitus.
- Hyvän ja pysyvän hoitotuloksen edellytyksenä ovat potilaan toimiva omahoito ja säännöllinen ylläpitohoito.
- Terveet hampaan kiinnityskudokset ovat tärkeä osa yleisterveyttä.
Tiivistelmä ja potilasversio
- Suosituksen tiivistelmä «Parodontiitti»1
- Suosituksen yleiskielinen potilasversio suomeksi «Hampaan kiinnityskudossairaus eli parodontiitti»2 ja ruotsiksi «Tandlossningssjukdom (parodontit)»3
Aiheen rajaus
- Suositus käsittelee hampaan kiinnityskudossairauksien ja peri-implanttisairauksien ehkäisyä, diagnostiikkaa ja ei-kirurgista hoitoa.
- Suosituksessa ei käsitellä
- hampaan kiinnityskudosten ja peri-implanttikudosten kirurgisia hoitomenetelmiä
- akuutteja parodontiumin infektioita lukuun ottamatta parodontiittiin liittyvää absessia ja endo-paroleesiota (ks. myös Käypä hoito -suositus Hammasperäiset äkilliset infektiot ja mikrobilääkkeet «Mikrobilääkkeet hammasperäisten infektioiden hoidossa ja komplikaatioiden ehkäisyssä»4, «Hammasperäiset äkilliset infektiot ja mikrobilääkk...»1)
- pitkäaikaissairauksien ilmentymiä hampaan kiinnityskudoksissa.
Tavoitteet
- Suosituksen tavoitteina on
- kiinnittää huomiota gingiviitin, parodontiitin ja peri-implanttisairauksien ehkäisyyn, diagnostiikkaan ja hoitoon sekä ylläpitohoitoon
- lisätä tietoisuutta hampaan kiinnityskudos- ja peri-implanttisairauksista, jotta ihmiset osaisivat hakeutua riittävän ajoissa hoitoon ja pystyisivät toimimaan aktiivisesti osana hoitotiimiä
- lisätä tietoisuutta parodontiitin vaikutuksista pitkäaikaissairauksiin
- esittää malli parodontiittia sairastavan potilaan toimivasta hoitopolusta.
Kohderyhmät
- Suosituksen kohderyhminä ovat
- hammaslääkärit, suuhygienistit ja suun terveydenhuollon muut ammattihenkilöt
- muut terveydenhuollon ammattihenkilöt (mm. lääkärit, neuvola- ja kouluterveydenhoitajat, opiskelu- ja työterveyshuollon ammattihenkilöt, diabeteshoitajat, vanhusten hoivatyötä tekevät)
- päättäjät, joilla on mahdollisuus vaikuttaa terveydenhuollon resursseihin
- potilasyhdistykset, kuten sydän-, diabetes- ja reumayhdistykset
- muu väestö.
Määritelmät
- Parodontiumilla tarkoitetaan hampaan kiinnityskudoksia ja parodontiitilla hampaan kiinnityskudossairautta.
- Suositukseen liittyvää alan termistöä on koottu lisätietoaineistoon «Käypä hoito -suositukseen Parodontiitti liittyviä määritelmiä»1.
Esiintyvyys
- Terve Suomi -tutkimuksen «Suominen L, Harjunmaa U. Suunterveyden tutkimus. T...»2 ja tutkimuksen julkaisemattoman aineiston mukaan gingiviitti ja parodontiitti ovat
merkittävä hammashoidollinen kansanterveysongelma 20 vuotta täyttäneillä hampaallisilla
suomalaisilla.
- Ienverenvuotoa yli 10 %:ssa hampaista esiintyy 91 %:lla (miehistä 95 %:lla ja naisista 88 %:lla).
- Syventyneitä (≥ 4 mm) ientaskuja (vähintään 1) esiintyy 74 %:lla (miehistä 81 %:lla
ja naisista 71 %:lla)
- 20–34-vuotiaista 64 %:lla
- 35–44-vuotiaista 73 %:lla.
- Syviä (≥ 6 mm) ientaskuja (vähintään 1) esiintyy 19 %:lla (miehistä 26 %:lla ja naisista
14 %:lla)
- 20–34-vuotiaista 8 %:lla
- 35–44-vuotiaista 18 %:lla.
- Kaikkien ikäluokkien tiedot ja tietoa Terve Suomi -tutkimuksen toteutuksesta löytyvät THL:n sivuilta «https://www.thl.fi/tervesuomi_verkkoraportit/ilmioraportit_2023/suunterveys_syventava_tutkimus.html»1.
- Terveys 2000- ja 2011 -tutkimuksiin verrattuna ientaskujen esiintyvyys on suurentunut «Terveys, toimintakyky ja hyvinvointi Suomessa 2011...»3. Myös nuorilla on nähtävissä merkkejä alkavasta parodontiitista «Nazir M, Al-Ansari A, Al-Khalifa K, ym. Global Pre...»4, «Heikkinen AM, Pajukanta R, Pitkäniemi J, ym. The e...»5. Parodontiitin esiintyvyys lisääntyy selkeästi jo alle 30-vuotiailla, erityisesti tupakoivilla «Tupakointi ilmeisesti lisää tupakoivien nuorten (15–25-vuotiaiden) alveoliluukadon riskiä, heiltä löytyy enemmän parodontiittiin liittyviä patogeenejä, ja heillä todetaan enemmän parodontiittia kuin samanikäisillä nuorilla, jotka eivät tupakoi.»B.
- Vaikean parodontiitin (vaiheet III–IV) esiintyvyys lisääntyy iän myötä siten, että ilmaantuvuus kasvaa jyrkästi 20. ja 40. ikävuoden välillä «Kassebaum NJ, Bernabé E, Dahiya M, ym. Global burd...»6.
- Maailmanlaajuisesti tarkasteltuna vaikean parodontiitin (vaiheet III–IV) esiintyvyys (11,2 %) ei muuttunut vuodesta 1990 vuoteen 2010 «Kassebaum NJ, Bernabé E, Dahiya M, ym. Global burd...»6, mutta se suureni vuosien 2010 ja 2020 välillä 24 %:iin «Trindade D, Carvalho R, Machado V, ym. Prevalence ...»7.
- Poski- ja etuhampaisiin paikallistuvan nopeasti etenevän parodontiitin esiintyvyys suomalaisessa väestössä on noin 0,1 % «Saxén L. Juvenile periodontitis in Finland. Proc F...»8. Kansainvälisesti sen esiintyvyys 3–20-vuotiailla on 0,6–1,6 % «Catunda RQ, Levin L, Kornerup I, ym. Prevalence of...»9.
- Implanteilla hoidetuista potilaista peri-implanttimukosiittia esiintyy keskimäärin 43–47 %:lla ja peri-implantiittia 20–34 %:lla «Jepsen S, Berglundh T, Genco R, ym. Primary preven...»10, «Derks J, Tomasi C. Peri-implant health and disease...»11, «Lee CT, Huang YW, Zhu L, ym. Prevalences of peri-i...»12, «Diaz P, Gonzalo E, Villagra LJG, ym. What is the p...»13, «Kordbacheh Changi K, Finkelstein J, Papapanou PN. ...»14.
- Altistavat tekijät vaikuttavat merkittävästi peri-implantiitin esiintyvyyteen «Reis INRD, do Amaral GCLS, Hassan MA, ym. The infl...»15, ks. taulukko «Peri-implanttisairauksille altistavia ja syytekijöitä ...»2.
Altistavat tekijät
- Riski sairastua parodontiittiin vaihtelee yksilöittäin.
- Altistavien tekijöiden huolellinen selvitys ja suurentuneen riskin yksilöiden löytäminen on tärkeää ehkäisyn ja hoidon kohdentamiseksi.
- Parodontiitille altistavia ja syytekijöitä luetellaan taulukossa «Parodontiitille ja sen uusiutumiselle altistavia ja syytekijöitä...»1. Lasten ja nuorten parodontiittia ennustavia merkkejä esitetään lisätietoaineiston taulukossa «Parodontiitin ennusmerkkejä lapsilla ja nuorilla»2.
- Peri-implanttisairauksille altistavia ja syytekijöitä luetellaan taulukossa «Peri-implanttisairauksille altistavia ja syytekijöitä ...»2. Riskinarviossa voidaan hyödyntää monitekijäistä riskianalyysityökalua (Implant Disease Risk Assessment, IDRA) ennen implantointia ja implantoinnin jälkeen, ks. «https://www.perio-tools.com/idra/en/»2.
Diagnostiikka
Tavoite
- Diagnostiikan tavoitteena on tunnistaa hampaita ja hammasimplantteja ympäröivissä
kudoksissa:
- tulehduksen merkit (punoitus, turvotus, verenvuoto taskumittauksen yhteydessä)
- syventyneet ien- tai implanttitaskut
- kliininen kiinnityskato
- röntgenkuvissa havaittava alveoliluukato.
- Diagnostiikan tavoitteena on myös tunnistaa taudin uusiutuminen parodontiittia sairastaneella potilaalla.
Oireet
- Ienverenvuoto (harjauksen tai hammasvälien puhdistuksen yhteydessä) on silmin havaittava
merkki tulehduksesta, ja myös ikenen punoitus ja turvotus ovat tavallisia (kuva «Tulehduksen merkkejä hampaanvieruskudoksen alueella»1). Samanlaisia tulehduksen merkkejä liittyy myös peri-implanttisarauksiin.
- Näkyvät tulehdusmerkit ovat tupakoivilla lievemmät kuin tupakoimattomilla «Tupakointi peittää parodontiitin kliinisiä merkkejä vähentämällä merkittävästi ienverenvuodon esiintymistä.»A.
- On huomattava, että tauti voi olla pitkään oireeton ja edellä mainitut tulehduksen merkit saattavat puuttua vaikeassakin parodontiitissa ja peri-implantiitissa.
- Hampaan lisääntynyt liikkuvuus, asentomuutokset (mm. siirtyminen ja rakojen muodostuminen) ja märkävuoto ientaskusta voivat liittyä vaikeaan (vaiheen III) tai pitkälle edenneeseen (vaiheen IV) parodontiittiin.
- Pahanhajuinen hengitys saattaa liittyä gingiviittiin ja parodontiittiin «Quirynen M, Dadamio J, Van den Velde S, ym. Charac...»93, «Sanz M, Bäumer A, Buduneli N, ym. Effect of profes...»94 sekä peri-implanttisairauksiin.
- Verenvuodon lisäksi voi esiintyä märkävuotoa.

Tulehduksen merkkejä hampaanvieruskudoksen alueella. © Tiina Varrela
Esitiedot
- Koska monet sairaudet tai niiden hoito voivat vaikuttaa parodontiittiin, peri-implantiittiin
ja niiden hoitoon, alkutilanteessa selvitetään ja kirjataan potilaan mahdolliset pitkäaikaissairaudet
ja niihin käytetty lääkitys. Tarvittaessa konsultoidaan lääkäriä.
- Esimerkiksi huonossa hoitotasapainossa oleva diabetes «Diabetesta sairastavilla on ilmeisesti suurempi riski sairastua parodontaalisairauksiin kuin niillä, jotka eivät sairasta diabetesta, ja huono hoitotasapaino ilmeisesti lisää riskiä.»B, «Poorly controlled diabetes mellitus may increase the risk for peri-implantitis.»C ja immuunipuutossairaudet «Holmstrup P, Glick M. Treatment of periodontal dis...»95 altistavat parodontiitille ja peri-implantiitille. Diabetespotilaan sokerihemoglobiini (HbA1c) on syytä selvittää ja ohjata potilas tarvittaessa diabeteshoitajalle tai lääkärille.
- Esitiedoista on tärkeä huomioida lääkitykset, jotka voivat aiheuttaa hoitotapahtumassa riskejä, esimerkiksi vuotokomplikaatioita tai interaktioita, tai lisätä infektioherkkyyttä. Monilääkitykset ja antiresorptiivinen lääkitys saattavat heikentää implanttien ennustetta «Fretwurst T, Nelson K. Influence of Medical and Ge...»76, «Tsaousoglou P, Chatzopoulos GS, Tsalikis L, ym. Pr...»96.
- Tietyt lääkeaineet, muun muassa immunosuppressiivinen siklosporiini, osa kohonneen verenpaineen hoidossa käytettävistä kalsiumkanavan salpaajista ja epilepsialääkkeistä muun muassa fenytoiini, voivat altistaa ikenen liikakasvulle «Bondon-Guitton E, Bagheri H, Montastruc JL. Drug-i...»97, «Glick A, Sista V, Johnson C. Oral Manifestations o...»98.
- Tupakointi: tupakoinnin kesto ja määrä vaikuttavat parodontiitin ja peri-implantiitin esiintymiseen, kudostuhon vaikeusasteeseen ja sen etenemiseen sekä hoidon ennusteeseen «Tupakointi huonontaa merkittävästi parodontiumin terveydentilaa, lisää alveoliluukatoa, heikentää parodontiumin paranemista ja suurentaa hampaiden menettäminen riskiä.»A, «Tupakointi ilmeisesti lisää tupakoivien nuorten (15–25-vuotiaiden) alveoliluukadon riskiä, heiltä löytyy enemmän parodontiittiin liittyviä patogeenejä, ja heillä todetaan enemmän parodontiittia kuin samanikäisillä nuorilla, jotka eivät tupakoi.»B, «Smoking, irregular supportive periodontal treatment (maintenance) and presence of periodontitis or periodontitis with poor response to treatment are significant risk factors for peri-implantitis and implant loss.»A.
- Omahoitotottumukset: riittävä päivittäinen suuhygienia edellyttää hampaiden ja hammasimplanttien harjauksen lisäksi hammasvälien puhdistamista «Jepsen S, Berglundh T, Genco R, ym. Primary preven...»10, «Sälzer S, Slot DE, Van der Weijden FA, ym. Efficac...»99.
- Aiempi hammashoito ja ylläpitohoidon säännöllisyys «Parodontiitin etenemistä ja hampaiden menetystä ylläpitohoidon aikana ennustavat potilaan tupakointi, epäsäännöllinen ylläpitohoidossa käynti, parodontiitin vaikeusaste alkutilanteessa ja jäännöstaskujen määrä ylläpitohoidon aikana.»A, «Smoking, irregular supportive periodontal treatment (maintenance) and presence of periodontitis or periodontitis with poor response to treatment are significant risk factors for peri-implantitis and implant loss.»A.
Kliininen tutkimus
- Hammaslääkäri tekee parodontologisen tutkimuksen jokaiselle suun terveydentilan tutkimuksen osana. Sama koskee suuhygienistin tekemää suun terveystarkastusta.
- Profylaktista mikrobilääkitystä tarvitseville annetaan tarvittava lääkitys ennen ien-
ja implanttitaskumittausta «Martins CC, Lockhart PB, Firmino RT, ym. Bacteremi...»100.
- Profylaksin tarve harkitaan potilaan infektiokomplikaatioriskin ja parodontologisen tilanteen mukaan.
- Toistuvien profylaksiannosten vähentämiseksi taskumittaus suositellaan tehtävän hoitokäynnin yhteydessä.
- Parodontiumin tilanne selvitetään kaikista hampaista ja hammasimplanteista.
- Viisaudenhammasalueella todetut syventyneet ientaskut saattavat vuosien mittaan ennustaa heikentyvää parodontaalitilannetta koko hampaiston alueella tai jo olemassa olevan parodontiitin etenemistä (ks. Käypä hoito -suositus Viisaudenhammas «Viisaudenhammas»5, «Viisaudenhammas. Käypä hoito -suositus. Suomalaise...»101), «Blakey GH, Marciani RD, Haug RH, ym. Periodontal p...»102, «Offenbacher S, Beck JD, Moss KL, ym. What are the ...»103.
- Lapsilla ja nuorilla parodontologinen tutkimus on syytä sisällyttää vähintään valtioneuvoston
asetuksen mukaisiin, tietyt ikäluokat kattaviin terveystarkastuksiin, joissa selvitetään
suun terveydentila ja hoidon tarve «Valtioneuvoston asetus neuvolatoiminnasta, koulu- ...»104, «http://www.finlex.fi/fi/laki/alkup/2011/20110338»3.
- Alle kouluikäisiltä ja ensimmäisen vuosiluokan oppilailta tutkitaan ja rekisteröidään plakki, hammaskivi ja ientulehdus.
- Edellä mainitun lisäksi kolmannesta vuosiluokasta alkaen oppilaille annetaan tietoa tupakka- ja nikotiinituotteiden haitoista ja oppilaita kannustetaan pidättäytymään näiden tuotteiden käytöstä, ks. Käypä hoito -suositus Tupakka- ja nikotiiniriippuvuuden ehkäisy ja hoito «Tupakka- ja nikotiiniriippuvuuden ehkäisy ja hoito»6, «Tupakka- ja nikotiiniriippuvuuden ehkäisy ja hoito...»105.
- Kahdeksannesta vuosiluokasta lähtien tehdään täydellinen parodontiumin tutkimus osana suun terveystarkastusta. Tämä koskee myös opiskeluterveydenhuoltoa.
- Oppilaiden suun terveystarkastuksiin sisältyy aina myös hammaslääkärin tutkimuksia, jotka kohdennetaan tarpeen mukaan.
- Pitkäaikaissairaudet tai niiden lääkitykset saattavat altistaa parodontaalisairauksille. Tutkimukset ja ehkäisevät toimenpiteet kohdistetaan suun terveydentila ja riskitekijät yksilöllisesti huomioiden. Tupakka- ja nikotiinituotteiden käytön ehkäisy ja vieroitus huomioidaan myös, ks. Hyvä käytäntö -konsensussuositus Suun tutkimus- ja hoitovälin määrittäminen «Suun tutkimus- ja hoitovälin määrittäminen Hyvä käytäntö -konsensussuositus»7, «Suun tutkimus- ja hoitovälin määrittäminen Hyvä kä...»106.
- Parodontologisessa tutkimuksessa rekisteröidään
- plakin sijainti (tai kuvaillaan plakin sijainti ja määrä sanallisesti potilasasiakirjaan)
- ien- ja implanttitaskumittauksen tulokset kuudelta pinnalta hammasta tai implanttia
kohden
- taskusyvyydet (≥ 4 mm) ja taskumittauksen jälkeinen verenvuoto, jotka on määritetty kaikista hampaista ja implanteista kuljettamalla ientaskumittaria askeltaen juuren tai implantin pintaa pitkin hampaan tai implantin akselin suuntaisesti
- mahdollinen märkävuoto
- kiinnityskadon määrä vaikeimmin vaurioituneilla alueilla kuvaillaan sanallisesti
- furkaatiovauriot
- furkaatioalueiden tutkimiseen tarvitaan furkaatiokoetin
- furkaatiovaurioista määritetään niiden aste (I–IV) ja sijainti «Nieminen M, Varrela T, Könönen E ym. Furkaatiolees...»107
- plakkiretentiot (hammaskivi, paikkojen ja kruunujen yli-/alimäärät, sementtiylimäärät, implanttipäällysrakenteisiin liittyvät seikat ja irrotettavat proteesit)
- hampaiden liikkuvuudet (sekä horisontaalisesti että vertikaalisesti, asteet 1–3), purennan liukuliikkeet ja hampaiden kosketussuhteet alaleuan eri asennoissa sekä purennan esikontaktit ja liikkuvuus purentafunktiossa (ks. Terveysportti, Hammaslääkärin tekemä suun perustutkimus «https://www.terveysportti.fi/apps/dtk/hat/article/hml00023?toc=3564»4, vaatii käyttöoikeuden)
- menetetyt hampaat (purentaparien lukumäärä)
- implanttifikstuuran liikkuvuus, joka on merkki koko osseointegraation menetyksestä (ja edellyttää implantin poistoa) «Lindhe J, Meyle J, Group D of European Workshop on...»108.
- Rekisteröinti tehdään käytössä olevaan potilastietojärjestelmään.
- Jos potilastietojärjestelmään ei ole mahdollista tehdä rekisteröintiä rakenteisesti, voidaan käyttää internetpohjaista ohjelmaa, esimerkiksi «http://www.periodontalchart-online.com/uk/index.asp»5.
- Tarvittaessa rekisteröidään tai kuvaillaan sanallisesti
- ienrajan kulku (ienvetäytymät ja ienliikakasvut)
- ikenen poikkeava muoto, väri ja pintarakenne
- ikenen ilmiasu (fenotyyppi; ikenen paksuus, keratinisoituneen ikenen leveys ja bukkaalisen luuseinämän paksuus) «Caton JG, Armitage G, Berglundh T, ym. A new class...»109, «Jepsen S, Caton JG, Albandar JM, ym. Periodontal m...»110 ja implanttia ympäröivän limakalvon ilmiasu «Avila-Ortiz G, Gonzalez-Martin O, Couso-Queiruga E...»111
- huulijänteen ja lihaskiinnikkeiden kiinnityskohdat silloin, kun ne liittyvät kudosmuutoksiin marginaalisen ikenen alueella
- hampaiden asentomuutokset.
- Tutkimuksessa on huomattava, että
- liian kevyesti tai voimakkaasti suoritettu ientaskumittaus johtaa hampaan kiinnityskudosten terveydentilan ali- tai yliarvioimiseen. On tärkeää, että mittaus suoritetaan standardoidusti «Larsen C, Barendregt DS, Slot DE, ym. Probing pres...»112, «Bulthuis HM, Barendregt DS, Timmerman MF, ym. Prob...»113. Mittaus ei tavallisesti aiheuta kipua potilaalle.
- manuaalisella ientaskumittauksella saavutetaan riittävä diagnostinen tarkkuus «Wang SF, Leknes KN, Zimmerman GJ, ym. Reproducibil...»114, «Grossi SG, Dunford RG, Ho A, ym. Sources of error ...»115
- ienverenvuoto on merkki tulehduksesta, ja se ennustaa parodontiitin syntyä ja etenemistä
«Ienverenvuoto ennustaa kiinnityskatoa ja sen etenemistä.»A
- Tupakoivilla verenvuotoprosentti ei yleensä anna luotettavaa kuvaa kiinnityskudosten tulehdusasteesta «Tupakointi peittää parodontiitin kliinisiä merkkejä vähentämällä merkittävästi ienverenvuodon esiintymistä.»A.
- Tupakoinnin lopettaneilla ienverenvuoto voi lisääntyä muutaman viikon ajaksi hyvästä omahoidosta huolimatta «Scott DA, Singer DL. Suppression of overt gingival...»116.
- Toistuvasti samassa kohdassa todettu ienverenvuoto ennustaa kiinnityksen menetystä «Schätzle M, Löe H, Ramseier CA, ym. Clinical cours...»56, ja sen puuttuminen on merkki terveestä parodontiumista «Lang NP, Adler R, Joss A, ym. Absence of bleeding ...»117.
- taskumittaus tehdään myös implanttien ympäriltä «Jepsen S, Berglundh T, Genco R, ym. Primary preven...»10, «Lindhe J, Meyle J, Group D of European Workshop on...»108
- Tavanomainen tutkimus ei vahingoita implantin pehmytkudoskiinnitystä eikä implantin pintaa.
- Jos implanttikruunun muoto estää mittauksen useammalta pinnalta, vähintään yksi pinta pitäisi saada mitatuksi. Tarvittaessa apuna voi käyttää furkaatiokoetinta.
- Verenvuoto taskumittauksen jälkeen on merkki peri-implanttikudoksen tulehduksesta ja viittaa peri-implanttimukosiittiin tai peri-implantiittiin.
Kuvantamistutkimukset
- Kun kliinisessä tutkimuksessa todetaan merkkejä parodontiitista tai peri-implantiitista, on syytä tehdä röntgenologinen tutkimus, josta laadittu lausunto liitetään potilasdokumentteihin.
- Panoraamatomografia antaa yleiskuvan alveoliluun määrästä ja luureunan kulusta (vertikaalinen/horisontaalinen luukato).
- Tarvittaessa sitä täydennetään suunsisäisin röntgenkuvin (periapikaalikuvat, bitewing-kuvat
tai pystysuuntaiset bitewing-kuvat), jotka ovat panoraamatomografiaa tarkempia luumuutosten,
kuten II–III asteen furkaatiovaurioiden, vertikaalisten luutaskujen ja implanttia
ympäröivän luukadon, havaitsemisessa «Pepelassi EA, Tsiklakis K, Diamanti-Kipioti A. Rad...»118, «Preshaw PM. Detection and diagnosis of periodontal...»119, «Graetz C, Plaumann A, Wiebe JF, ym. Periodontal pr...»120, (kuva «Alkava parodontiitti nuorella potilaalla»2).
- Röntgenkuvien kyky osoittaa lievää kudostuhoa (alle 2 mm) marginaalisen luun alueella on heikko «Whaites E, Drage N. Essentials at Dental Radiograp...»121.
- Jos marginaalisen luun ja kiille-sementtirajan välinen etäisyys on yli 2 mm, löydös viittaa parodontiittiin
- Mikäli implantin kohdalla havaitaan edennyttä luukatoa tai arvioidusta lähtötilanteen luurajasta luukatoa ≥ 3 mm, löydös viittaa peri-implantiittiin.
- Bitewing-röntgenkuvat on tulkittava huolellisesti marginaalisen luurajan kulun arvioimiseksi ja approksimaalisen hammaskiven toteamiseksi «Bitewing-röntgenkuvista rekisteröidään marginaalisen luutason menetys ja hammaskivi, koska ne ovat ilmeisesti parodontiitin merkkejä.»B. Bitewing-kuvista on tärkeää tarkastella luun epätarkkarajaisuutta ja luun tiheyden vähenemistä kauttaaltaan «Whaites E, Drage N. Essentials at Dental Radiograp...»121, (kuva «Alkava parodontiitti nuorella potilaalla»2).
- Pystysuuntaiset bitewing-kuvat voivat olla tarpeen alveoliluukadon havainnoinnissa parodontiitin vaiheissa III ja IV «Whaites E, Drage N. Essentials at Dental Radiograp...»121, ks. kuva «Pystysuuntaiset bitewing-kuvat vaiheen III parodontiitissa»3.
- Laajentunut parodontaalirako ja vertikaalinen tai furkaatioalueen luukato voivat viitata purentatraumaan.
- Implantin ympärillä luukato on yleensä maljamainen.
- Lasten ja nuorten poski- ja etuhampaisiin paikallistuva nopeasti etenevä parodontiitti on diagnosoitavissa alveoliluun vertikaalisesta kadosta ensimmäisten poskihampaiden
ja etuhampaiden approksimaaliväleistä.
- Jos ensimmäisen poskihampaan kohdalla on muutoksia luurajassa, on syytä ottaa tarkennuskuva etuhammasalueilta.
- Kartiokeilatietokonetomografia ei kuulu parodontologiseen perustutkimukseen. Erityistapauksissa se voi tulla kyseeseen luutaskujen tai furkaatiovaurioiden tarkemmassa diagnostiikassa.

Alkava parodontiitti nuorella potilaalla. Marginaalinen luuraja kuvautuu hieman epätarkkana.
© Suun erikoishoidon yksikkö, Helsingin kaupunki
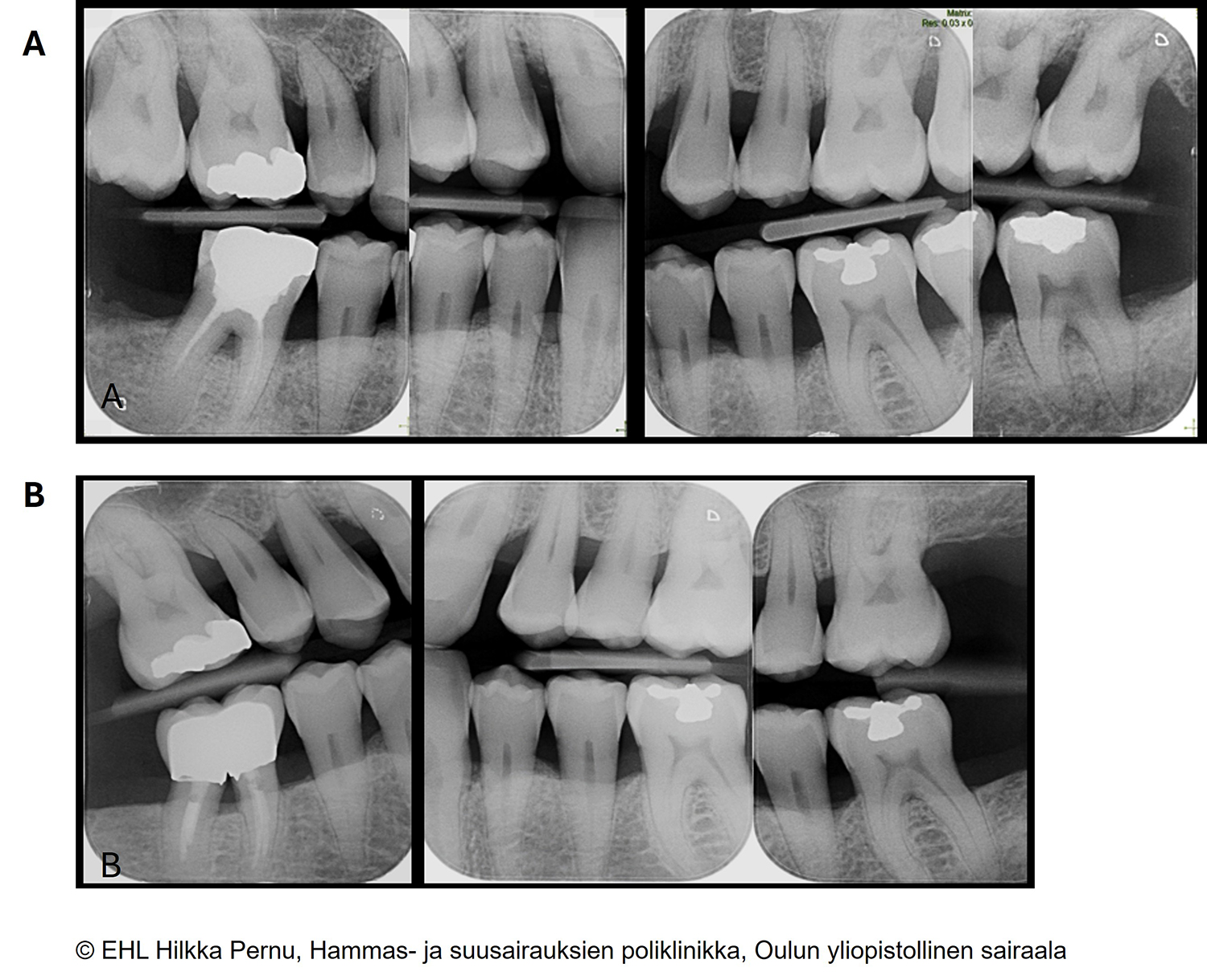
Pystysuuntaiset bitewing-kuvat vaiheen III parodontiitissa.
A) Hoitoontulotilanteessa 65-vuotiaan potilaan komplisoitunut parodontiitti; pitkälle edennyt laaja-alainen luukato, vertikaalisia luutaskuja, furkaatiovaurioita ja sekundaariseen purentatraumaan viittaavia muutoksia.
B) Kokonaishoitovasteen arviointitilanteen kuvat kahden vuoden kuluttua. Marginaalinen luuraja kuvautuu tarkkarajaisena, ja alkutilanteeseen nähden luutaskuissa ja furkaatiovaurioissa on saavutettu regeneraatiota.
Täydentävät diagnostiset tutkimukset
- Mikrobiologista tutkimusta ei tarvita rutiinimaisesti parodontologisessa diagnostiikassa.
- Mikrobiologinen näyte suositellaan otettavaksi
- aina, kun suunnitellaan mikrobilääkitystä parodontiitin hoidossa
- nuorilta (alle 30-vuotiailta), kun kyseessä on hampaan kiinnityskudosten nopeasti edennyt paikallinen tuho tai kun parodontiittia esiintyy laajalla alueella
- aikuisilta, kun parodontiitti on edennyt nopeasti tai kun vaste asianmukaiseen hoitoon on huono.
- Ien- tai implanttitaskun biofilmi on yleisimmin käytetty mikrobiologinen näyte.
- Näytteestä määritetään keskeiset parodontiittiin liittyvät patogeenit.
- Tulosten tulkinnassa käytetään eri bakteerilajeille määritettyjä merkitsevyysrajoja.
- Sieniviljelynäyte voidaan ottaa, jos epäillään sieni-infektiota ikenen alueella.
- Useita biomarkkereita on tutkittu, mutta toistaiseksi ei ole menetelmää, joka korvaisi parodontologisen tutkimuksen tai vaikuttaisi kliinisiin hoitokäytäntöihin «Wei S, Lin T, Sáenz-Ravello G, ym. Diagnostic accu...»122, «Deng K, Pelekos G, Jin L, ym. Diagnostic accuracy ...»123, «Buduneli N, Bıyıkoğlu B, Kinane DF. Utility of gin...»124, «Ebersole JL, Hasturk H, Huber M, ym. Realizing the...»125.
- Kudosnäytettä voidaan tarvita erotusdiagnostiikassa, jos epäillään ikenen alueella ilmenevää limakalvosairautta «Holmstrup P, Plemons J, Meyle J. Non-plaque-induce...»126.
- Hematologiset laboratoriotutkimukset voivat tulla kyseeseen, jos epäillään esimerkiksi sokeritasapainon ja veren hyytymisen häiriöitä tai pitkäaikaissairauksia.
Keskeiset diagnoosit
- Löydösten perusteella asetetaan parodontologinen diagnoosi ja parodontiittitapauksissa määritetään taudin vaihe (I–IV), laajuus (yleistynyt / paikallistunut / poski- ja etuhampaisiin paikallistuva) ja potilaan riskiluokka (A–C).
- Tavallisimmat diagnoosit esitetään taulukossa «Hampaita ja hammasimplantteja ympäröivien kudosten sairaudet (ICD-10-tautiluokitus). Diagnoosikoodi K05.4 vastaa tässä suosituksessa käytettyä uudempaa termiä poski- ja etuhampaisiin paikallistuva parodontiitti....»3.
- Kliinisesti terveen parodontiumin «Chapple ILC, Mealey BL, Van Dyke TE, ym. Periodont...»127 sekä plakkivälitteisen gingiviitin «Trombelli L, Farina R, Silva CO, ym. Plaque-induce...»128 diagnostiset kriteerit löytyvät lisätietoaineistosta «Kliinisesti terveen parodontiumin sekä plakkivälitteisen gingiviitin diagnostiset kriteerit»3. Gingiviitin diagnoosi voidaan asettaa, kun hampaistossa todetaan ienverenvuotoa
taskumittauksen yhteydessä vähintään 10 %:lla pinnoista «Trombelli L, Farina R, Silva CO, ym. Plaque-induce...»128, mutta ei kiinnityskatoa.
- Kun ienverenvuotoprosentti on 10–30, kyseessä on paikallinen gingiviitti. Kun se on yli 30, kyseessä on yleistynyt gingiviitti.
- Myös hoidetulla parodontiittipotilaalla, jolla on luukatoa ja kiinnityskatoa, diagnoosina voi olla gingiviitti (tällöin ienverenvuotoa voi esiintyä ainoastaan kohdissa, joissa taskusyvyys on alle 4 mm).
- Syventynyt ien- tai implanttitasku, kliininen kiinnityskato ja röntgenkuvasta havaittu alveoliluukato ovat parodontiitin ja peri-implantiitin diagnostisia merkkejä.
- Parodontiitti tulee diagnoosiksi, kun vähintään kahdessa ei-vierekkäisessä hampaassa
todetaan kliinisesti kiinnityskatoa tai röntgenologisesti luukatoa, syventynyt ientasku
(≥ 4 mm) ja verenvuotoa taskumittauksen yhteydessä «Papapanou PN, Sanz M, Buduneli N, ym. Periodontiti...»129, «Tonetti MS, Greenwell H, Kornman KS. Staging and g...»130.
- Jos parodontiittiin viittaavia löydöksiä esiintyy yksittäisessä hampaassa, erotusdiagnostiikkaan on kiinnitettävä erityistä huomiota.
- Parodontiittia voivat komplisoida paikalliset tekijät (vaikea ja pitkälle edennyt parodontiitti, vaiheet III ja IV). Ks. taulukko «Parodontiitin vaiheen määrittäminen , ....»4. On tarkoin harkittava, suurentaako yksittäisessä hampaassa esiintyvä komplisoiva tekijä parodontiitin vaihetta.
- Peri-implanttimukosiitti tulee diagnoosiksi, kun taskumittauksessa todetaan verenvuotoa useammasta kuin yhdestä kohtaa implantin ympäriltä tai märkävuotoa, mutta ei patologista luukatoa.
- Peri-implantiitti tulee diagnoosiksi, kun kliininen taskusyvyys on aiempiin mittauksiin
verrattuna suurentunut, siihen liittyy verenvuotoa (ja mahdollisesti märkävuotoa)
ja röntgenkuvissa havaitaan poikkeavaa alveoliluun katoa verrattuna proteettisen rakenteen
valmistumisvaiheen mittauksiin «Berglundh T, Armitage G, Araujo MG, ym. Peri-impla...»131, «Renvert S, Persson GR, Pirih FQ, ym. Peri-implant ...»132.
- Jos käytettävissä ei ole alkutilanteen tietoja tai muita aiempia tietoja, peri-implantiittidiagnoosi voidaan asettaa, kun todetaan verenvuotoa tai märkävuotoa, ≥ 6 mm syvä tasku ja luukatoa ≥ 3 mm «Herrera D, Berglundh T, Schwarz F, ym. Prevention ...»88.
Erotusdiagnostiikka
- Ientaskun ≥ 4 mm:n syvyys voi johtua hampaan kiinnityskadosta tai tulehduksen aiheuttamasta
turvotuksesta.
- Puberteetti «Mombelli A, Gusberti FA, van Oosten MA, ym. Gingiv...»133, «Nakagawa S, Fujii H, Machida Y, ym. A longitudinal...»134, raskaus «Figuero E, Carrillo-de-Albornoz A, Martín C, ym. E...»135, «Gürsoy M, Pajukanta R, Sorsa T, ym. Clinical chang...»136 ja tietyt lääkkeet «Trackman PC, Kantarci A. Connective tissue metabol...»137, «Seymour RA. Effects of medications on the periodon...»138, kuten kalsiumkanavan salpaajat ja immunosuppressiivit, voivat aiheuttaa ikenen turvotusta tai liikakasvua ilman kiinnityskatoa.
- Ienvetäytymä voi olla merkki parodontiitin aiheuttamasta kiinnityskadosta mutta myös seurausta mekaanisesta vauriosta, kuten harjaus- tai purentatraumasta, tai traumaattisesta purennasta.
- Paikallisesti syventynyt ientasku ja kiinnityskato tai märkävuoto voivat johtua paitsi parodontiitista myös esimerkiksi hampaan juuren murtumasta tai apikaalialueen tulehduksesta.
- Pehmytkudoksen vetäytymä implantin ympärillä voi liittyä liian bukkaalisesti tai oraalisesti asetettuun implanttiin ja ohueen fenotyyppiin. Se voi johtua myös marginaalisesta luukadosta, jonka syynä voi olla fysiologinen luun muotoutuminen tai hoidettu peri-implantiitti.
- Fisteli implantin kohdalla voi olla merkki teknisestä komplikaatiosta, kuten löystyneestä abutmenttiruuvista.
| K05 | Hampaan kiinnityskudossairaudet |
| K05.0 | Äkillinen ientulehdus |
| K05.1 | Pitkäaikainen ientulehdus |
| K05.10 | Pitkäaikainen komplisoitumaton ientulehdus |
| K05.11 | Pitkäaikainen hyperplastinen ientulehdus |
| K05.12 | Pitkäaikainen haavainen ientulehdus |
| Muut ikenen tulehdukset | |
| A69.1 | Kuolioituva haavainen ientulehdus (nekrotisoiva gingiviitti) |
| O26.80 | Raskauteen liittyvä ientulehdus |
| K05.2 | Äkillinen parodontiitti |
| K05.20 | Ienperäinen parodontaalinen absessi, jossa ei avannetta |
| K05.21 | Ienperäinen parodontaalinen absessi, jossa avanne |
| K05.3 | Pitkäaikainen parodontiitti |
| K05.30 | Komplisoitumaton parodontiitti |
| K05.31 | Komplisoitunut parodontiitti |
| K05.32 | Pitkäaikainen perikoroniitti |
| K05.4 | Parodontoosi (poski- ja etuhampaisiin paikallistuva parodontiitti) |
| K06 | Muut ikenien sairaudet |
| K06.00 | Paikallinen ikenen vetäytyminen |
| K06.01 | Yleinen ikenen vetäytyminen |
| K06.1 | Ikenen liikakasvu |
| K06.2 | Ikenien traumaattiset vauriot |
| K06.20 | Traumaattisen purennan aiheuttama ikenen ärsytyshyperplasia |
| K06.21 | Hammasharjauksen aiheuttama ientrauma |
| T84 | Ortopedisten implanttien ja siirteiden komplikaatiot Y88.3 Lääketieteellisen toimenpiteen jälkeen ilmenneet pitkäaikaiset haittavaikutukset ja myöhemmät komplikaatiot |
| T84.60 | Hammasimplanttiin liittyvä tulehdus (peri-implanttimukosiitti) |
| T84.61 | Hammasimplanttiin liittyvä pehmytkudoksen liikakasvu |
| T84.62 | Hammasimplanttiin liittyvä ostiitti (peri-implantiitti) |
Taulukon tulostettava PDF-versio «hoi50086a.pdf»1
Parodontiitin vaihe, laajuus ja riskiluokka
- Parodontiittidiagnoosin jälkeen määritetään taudin vaihe, laajuus ja potilaan riskiluokka. Näiden perusteella laaditaan hoitosuunnitelma ja arvioidaan hoidon ennuste «Tonetti MS, Sanz M. Implementation of the new clas...»139.
- Parodontiitin vaihe ilmentää taudin vaikeusastetta, ja se määritetään ensisijaisesti
vaikeimmin vaurioituneiden kohtien kiinnityksen menetyksen tai röntgenologisesti määritetyn
luukadon perusteella (taulukko «Parodontiitin vaiheen määrittäminen , ....»4) «Papapanou PN, Sanz M, Buduneli N, ym. Periodontiti...»129, «Tonetti MS, Greenwell H, Kornman KS. Staging and g...»130. Lisäksi vaikeusastetta voivat nostaa muun muassa ientaskusyvyys, furkaatiovauriot
ja hampaiden lisääntynyt liikkuvuus.
- Alkavassa (vaihe I) ja keskivaikeassa (vaihe II) parodontiitissa esiintyy pääasiassa horisontaalista luukatoa juuren koronaalisessa kolmanneksessa (vaihe I: < 15 % ja vaihe II: 15–33 %) ja kliinistä kiinnityskatoa (vaihe I: 1–2 mm ja vaihe II: 3–4 mm) sekä < 6 mm:n ientaskuja.
- Alkavassa vaiheessa todetun parodontiitin (vaihe I) hoitoennuste on lähes aina hyvä.
- Vaikeassa parodontiitissa (vaihe III) ilmenee II vaiheen löydösten lisäksi vähintään yksi seuraavista löydöksistä: kiinnityskatoa on ≥ 5 mm, luukato on edennyt juuren keski- tai apikaalikolmannekseen, syventyneitä (≥ 6 mm) ientaskuja tai hampaistossa esiintyy II–III asteen furkaatiovaurioita tai vertikaalisia luutaskuja.
- Pitkälle edenneessä parodontiitissa (vaihe IV) on lisäksi menetetty parodontiitin seurauksena useita (≥ 5) hampaita ja ilmenee vähintään yksi seuraavista löydöksistä: hampaiden lukumäärä on < 20 (purentaparien määrä < 10), hampaissa esiintyy lisääntynyttä liikkuvuutta (2.–3. aste) tai purenta on vaarassa romahtaa. Vaiheen IV parodontiitti on yleistynyt.
- Taudin laajuus ilmentää taudin jakautumista hampaistossa. Se määritetään niiden hampaiden
prosentuaalisena osuutena, jotka täyttävät parodontiitin vaiheen vaikeuskriteerit
(kaikkein pisimmälle edenneessä vaiheessa):
- Kun hampaista on affisioitunut < 30 %, on kyseessä taudin paikallistunut muoto, ja kun ≥ 30 % on affisioitunut, on kyseessä taudin yleistynyt muoto.
- Paikallistuneessa muodossa arvioidaan myös kokonaistilanne. Jos potilaalla on esimerkiksi paikallistunut vaiheen III parodontiitti ja muualla hampaistossa parodontiitti on lievempiasteinen, tulee diagnoosiin tarkentaa kuvaus muun hampaiston tilanteesta «Kornman KS, Papapanou PN. Clinical application of ...»141
- Kyseessä voi olla myös poski- ja etuhampaisiin paikallistuva parodontiitti «Fine DH, Patil AG, Loos BG. Classification and dia...»140.
- Potilaan riskiluokka (A–C) määritetään kiinnitys- tai luukadon etenemisen perusteella
(taulukko «Potilaan riskiluokka ilmentää parodontiitin etenemisnopeutta huomioiden mahdolliset
riskitekijät taudin etenemiselle / puutteelliselle hoitovasteelle , . ...»5).
- Suora näyttö taudin etenemisestä on saatavissa aiemmista kirjauksista tai röntgenkuvista edeltävien viiden vuoden ajalta. Vaihtoehtoisesti riskiluokka voidaan määrittää radiologisen luukadon perusteella suhteutettuna ikään (epäsuora näyttö taudin etenemisestä). Arviointiperusteena käytetään hammasta, jossa on eniten luukatoa.
- Potilaan riskiluokkaa voivat nostaa tupakointi ja diabetes (luokat B–C).
- Tupakoinnin määrä < 10 tai ≥ 10 savuketta/vrk
- Pitkäaikaisverensokeriarvo (HbA1c) < 7 % tai ≥ 7 % (< 53 mmol/mol tai ≥ 53 mmol/mol)
- Lisäksi plakin vähäinen määrä nopeasti edenneen taudin yhteydessä viittaa suurentuneeseen riskiin (luokka C).
| Tyypillisiä kliinisiä löydöksiä | Röntgenologiset löydökset | |||||
|---|---|---|---|---|---|---|
| * prosentuaalinen osuus juuren pituudesta ** parodontiittia komplisoiva löydös ‡ parodontiitin vuoksi menetettyjen hampaiden lukumäärä |
||||||
| Parodontiitin vaihe | Erityispiirteet | Ienverenvuoto | Taskusyvyydet | Kiinnityskato | Puuttuvat hampaat ‡ | Luukato |
| alkava (vaihe I) | Lähinnä horisontaalista luukatoa | + | 4 mm | 1–2 mm | 0 | juuren koronaalikolmannes (< 15 %*) |
| keskivaikea (vaihe II) | Lähinnä horisontaalista luukatoa | + | 4–5 mm | 3–4 mm | 0 | juuren koronaalikolmannes (15–33 %*) |
| vaikea (vaihe III) | Edellisen lisäksi: vertikaalista luukatoa ≥ 3 mm** FII–III furkaatiovauriot** kohtalaiset vauriot alveoliharjanteella** |
+ | ≥ 6 mm** | ≥ 5 mm | 1–4 | juuren keski- tai apikaalikolmannes |
| pitkälle edennyt (vaihe IV) | Edellisen lisäksi vähintään yksi seuraavista:
|
+ | ≥ 6 mm** | ≥ 5 mm | ≥ 5 | juuren keski- tai apikaalikolmannes |
Taulukon tulostettava PDF-versio «hoi50086b.pdf»2
| Luokituksen primaarikriteerit | Luokitusta modifioivat tekijät | |||
|---|---|---|---|---|
| * luokitus määritetään ensisijaisesti kiinnitys- tai luukadon mukaan, kun ko. tieto
on saatavilla (suora näyttö taudin etenemisestä) ** määritetään hampaasta, jossa eniten röntgenologista luukatoa (epäsuora näyttö taudin etenemisestä) *** tupakointi ja diabetes voivat nostaa primaarikriteerein määritettyä riskiluokkaa, joten tupakoinnin määrä ja pitkäaikaisverensokeriarvo (HbA1c) huomioidaan riskiluokan määrityksessä |
||||
| Potilaan riskiluokitus | Kiinnitys- tai luukato edeltävien 5 vuoden aikana* | % luukato/ikä** | Tupakointi*** | Diabetes*** |
| Luokka A: Hidas taudin eteneminen |
Ei havaittavissa | < 0,50 | Savuttomuus | Normoglykeeminen potilas (HbA1c < 6,5 %, < 47 mmol/mol) |
| Luokka B: Kohtalainen taudin eteneminen |
< 2 mm | 0,50–1,0 | Tupakointi (< 10 savuketta/vrk) | Diabetesta sairastava potilas (HbA1c < 7,0 %, < 53 mmmol/mol) |
| Luokka C: Nopea taudin eteneminen |
≥ 2 mm | > 1,0 | Tupakointi (≥ 10 savuketta/vrk) | Diabetesta sairastava potilas (HbA1c ≥ 7,0 %, ≥ 53 mmol/mol) |
Taulukon tulostettava PDF-versio «hoi50086c.pdf»3
Ehkäisy
- Hyvä päivittäinen suuhygienia ehkäisee kaikenikäisten gingiviittiä ja parodontiittia «Sanz M, Herrera D, Kebschull M, ym. Treatment of s...»143. Lisäksi se ehkäisee peri-implanttimukosiittia ja peri-implantiittia «Renvert S, Quirynen M. Risk indicators for peri-im...»75, «Herrera D, Berglundh T, Schwarz F, ym. Prevention ...»88.
- Tehokas omahoito perustuu ensisijaisesti päivittäiseen hampaiden, hammasvälien ja
proteettisten rakenteiden puhdistukseen, jonka toteuttaminen ohjataan yksilöllisesti.
- Hampaansa vähintään 2 kertaa päivässä harjaavilla esiintyy vähemmän gingiviittiä ja parodontiittia kuin hampaansa harvemmin harjaavilla «Kansanterveyslaitos. Suomalaisten aikuisten suunte...»26.
- Sähköhammasharja vähentää plakkia ja gingiviittiä tehokkaammin kuin tavallinen hammasharja «Sähköhammasharjat poistavat tehokkaammin plakkia ja vähentävät tehokkaammin ientulehdusta kuin tavalliset hammasharjat.»A. Sähköhammasharjaa säännöllisesti käyttävien suun terveys on ilmeisesti parempi myös pitkäaikaisseurannassa «Pitchika V, Pink C, Völzke H, ym. Long-term impact...»144. Sähköhammasharja soveltuu myös lasten hampaiden harjaukseen ja on tehokkaampi kuin tavallinen hammasharja «Davidovich E, Shafir S, Shay B, ym. Plaque Removal...»145. Lapsen hampaiden harjaus on huoltajien vastuulla siihen asti, kunnes lapsen motoriikka on riittävä. Vaikka lapsi harjaisikin jo itse, on vielä alakouluikäisen harjaustulos usein tarpeen tarkastaa.
- Hammasvälien puhdistus on oleellinen osa päivittäistä omahoitoa, sillä parodontiitti alkaa usein taka-alueen hammasväleistä «Löe H, Morrison E. Periodontal health and disease ...»146.
- Suun terveydenhuollon ammattihenkilö valitsee potilaan kanssa sopivat puhdistusvälineet
yksilöllisen tarpeen ja hammasvälien koon mukaisesti «Tonetti MS, Chapple IL, Jepsen S, ym. Primary and ...»147.
- Lasten hammasvälien puhdistus opetetaan vanhemmille, jos hammasväleissä todetaan ientulehdusta. Hammaslanka on usein ensisijainen menetelmä lasten ja nuorten hammasvälien puhdistukseen. Lankaus soveltuu myös aikuisille, joilla ei ole kiinnityskudoskatoa tai joiden hammasvälit ovat tiiviit «Cepeda MS, Weinstein R, Blacketer C, ym. Associati...»38, «Sälzer S, Slot DE, Van der Weijden FA, ym. Efficac...»99.
- Hammaslangan käyttö hampaiden harjauksen yhteydessä poistaa tehokkaammin bakteeripeitteitä kuin pelkkä harjaus «Sambunjak D, Nickerson JW, Poklepovic T, ym. Floss...»148.
- Harjatikun käyttö on osoittautunut hoitomyöntyvyyden kannalta helposti omaksuttavaksi, ja sen teho poistaa plakkia hammasväleistä on parempi kuin pelkän harjauksen «van der Weijden F, Slot DE, van der Sluijs E, ym. ...»149, «Sälzer S, Graetz C, Dörfer CE, ym. Contemporary pr...»150, «Yost KG, Mallatt ME, Liebman J. Interproximal ging...»151, «Abouassi T, Woelber JP, Holst K, ym. Clinical effi...»152.
- Isoissa hammasväleissä ja pardontiittipotilailla parodontiitin uusimisen ehkäisyssä hammasväliharjat ovat usein tehokkain tapa puhdistaa hammasvälit «Slot DE, Valkenburg C, Van der Weijden GAF. Mechan...»153
- Implanttien puhdistukseen valitaan yksilölliset puhdistusvälineet proteettisten rakenteiden mukaan.
- Säännöllisesti hammasvälit puhdistavilla on vähemmän peri-implantiittia kuin niillä, jotka eivät puhdista hammasvälejä säännöllisesti «Romandini M, Lima C, Pedrinaci I, ym. Prevalence a...»81.
- Päivittäinen hampaiden harjaus tinafluoridia tai vähintään 50 % natriumbikarbonaattia sisältävällä hammastahnalla ilmeisesti vähentää aikuisten plakin määrää ja ientulehdusta «Päivittäinen hampaiden harjaus tinafluoridia tai 67 % natriumbikarbonaattia sisältävällä hammastahnalla saattaa vähentää plakin määrää hampaiden pinnoilla ja ientulehduksen oireita tehokkaammin kuin tavanomainen fluorihammastahna.»C, «Taschieri S, Tumedei M, Francetti L, ym. Efficacy ...»154, «Valkenburg C, Van der Weijden FA, Slot DE. Plaque ...»155.
- Savuttomuuteen kannustaminen ja tupakkatuotteista vieroittaminen kuuluvat kaikenikäisten parodontiitin ehkäisyyn «Tupakoinnin lopettaneilla ientaskut paranevat paremmin ja luukadon eteneminen hidastuu verrattuna tupakoitsijoihin.»A, «Lindson N, Thompson TP, Ferrey A, ym. Motivational...»156, «Ramseier CA, Suvan JE. Behaviour change counsellin...»157.
- Uusien nikotiinituotteiden käytön vaikutuksista kiinnityskudoksiin on vielä hyvin vähän tietoa. Nikotiini vaikuttaa paikallisesti limakalvon ja parodontiumin kudoksiin. Nuuskan käyttöön verrattavaa limakalvon paksuuntumista ja haavautumista sekä ikenen vetäytymistä on kokemusperäisesti todettu myös nikotiinipussien käyttäjillä. Nikotiinituotteiden käytön ehkäisy on osa suusairauksien ehkäisyä.
- Motivoivaa keskustelua voidaan käyttää omahoidon ohjauksessa motivaation lisäämiseksi «Motivoiva keskustelu saattaa olla tavanomaista omahoidon ohjausmenetelmää tehokkaampi ja saattaa parantaa sitä tehokkaammin suuhygieniatottumuksia, vähentää plakin määrää ja ienverenvuotoa.»C, «Werner H, Hakeberg M, Dahlström L, ym. Psychologic...»158 ja savuttomuuteen ja nikotiinittomuuteen kannustamisessa «Lindson N, Thompson TP, Ferrey A, ym. Motivational...»156. Ks. videot motivoivasta haastattelusta «Videot: Motivoiva haastattelu»4.
- Ammattimainen hampaiston puhdistus ja omahoidon ohjaus vähentävät bakteeripeitteitä hampaiden pinnoilla, ienverenvuotoa ja ikenien liikakasvua. Pelkän ammattimaisen puhdistuksen merkitys ilman omahoidon ohjausta on kyseenalainen «Hugoson A, Lundgren D, Asklöw B, ym. Effect of thr...»159, «Hujoel PP, Cunha-Cruz J, Loesche WJ, ym. Personal ...»160, «Needleman I, Nibali L, Di Iorio A. Professional me...»161.
- Implanttihoitoa edeltävä omahoitosuunnitelma ja perusteellinen parodontologinen tutkimus
sekä tarvittaessa hoito ovat oleellisia implanttikomplikaatioiden ehkäisyssä. Hoidon
suunnittelussa pitää huomioida potilaan parodontiittitausta sekä riskitekijöistä erityisesti
tupakointi, huonossa hoitotasapainossa oleva diabetes ja epäsäännöllinen ylläpitohoito
«Smoking, irregular supportive periodontal treatment (maintenance) and presence of periodontitis or periodontitis with poor response to treatment are significant risk factors for peri-implantitis and implant loss.»A. Ks. myös Vältä viisaasti -suositus «Implanttihoidot parodontiittipotilailla»5.
- Implanttipotilasta tulee kannustaa savuttomana pysymiseen ja diabetesta sairastavaa potilasta sairauden hyvän hoitotasapainon ylläpitämiseen «Heitz-Mayfield LJA, Salvi GE. Peri-implant mucosit...»80, «Gómez-Moreno G, Aguilar-Salvatierra A, Rubio Roldá...»162.
- Implanttien ammattimainen puhdistus omahoidon ohjauksen lisäksi vähentää peri-implanttimukosiittia «Gómez-Moreno G, Aguilar-Salvatierra A, Rubio Roldá...»162. Implanttien sijainti ja niiden varaan kiinnitettävät rakenteet on suunniteltava niin, että implanttien puhdistus on mahdollista.
- Implanttien säännöllinen ylläpitohoito on tärkeää peri-implanttisairauksien ehkäisemiseksi. Hoitoväli määräytyy potilaan riskiprofiilin mukaan «Monje A, Aranda L, Diaz KT, ym. Impact of Maintena...»163, taulukko «Peri-implanttisairauksille altistavia ja syytekijöitä ...»2.
- Peri-implantiitin ilmaantuvuus lisääntyy, kun ylläpitohoitoväli on yli 6 kuukautta «Monje A, Aranda L, Diaz KT, ym. Impact of Maintena...»163.
- Suun terveydenhuollon ammattihenkilöiden lisäksi koulu-, opiskelija- ja työterveyshuolto
voivat osallistua iensairauksien ehkäisyyn ja hoitoon monin tavoin, muun muassa
- kysymällä terveystarkastusten yhteydessä suun terveyteen liittyvistä asioista ja ohjaamalla tarvittaessa suun terveydenhuoltoon
- antamalla ohjeita suun hoidosta ja terveellisistä elintavoista, kuten tupakka- ja nikotiinituotteiden käytön lopettamisesta ja terveellisestä ruokavaliosta.
Gingiviitin ja peri-implanttimukosiitin hoito
- Gingiviitin ja peri-implanttimukosiitin hoidon tavoitteena on edistää parodontaaliterveyttä
ja estää parodontiitin ja peri-implantiitin synty.
- Hoitoon kuuluvat ammattimainen hampaiston puhdistus ja omahoidon ohjaus.
- Omahoidon ohjauksen tavoitteena on ohjata hampaiden ja implanttien puhdistus yksilöllisesti siihen parhaiten soveltuvilla välineillä.
- Omahoidon ohjauksessa keskitytään erityisesti niihin kohtiin, joissa tulehdusta on todettu.
- Usein on tarpeen opastaa hammasvälien puhdistukseen sopiva väline, ks. suosituksen kohta Ehkäisy «A1»2.
- Olennaista hoidon onnistumisen kannalta on päivittäinen huolellinen omahoito.
- Peri-implanttimukosiitin hoitoon tarvitaan siihen soveltuvat instrumentit (esim. titaani-instrumentit, implanttien puhdistukseen tarkoitetut ultraäänilaitteen kärjet, jauhepuhdistin tai harjat ja kumikupit) sekä tarvittaessa proteettisen päällysrakenteen irrottaminen ja muotoilu puhdistamisen helpottamiseksi «Jepsen S, Berglundh T, Genco R, ym. Primary preven...»10. Lisäksi opastetaan hammasvälien puhdistus «Herrera D, Berglundh T, Schwarz F, ym. Prevention ...»88, «Verket A, Koldsland OC, Bunaes D, ym. Non-surgical...»164, «Romandini M, Lima C, Pedrinaci I, ym. Prevalence a...»165.
- Gingiviitin hoitovaste arvioidaan noin kuukauden kuluttua.
- Gingiviitin hoitovasteen arviointiin käytetään hoidon jälkeen mitattua ienverenvuotoprosenttia.
- Hoidon tavoitteena on ienverenvuoto < 10 % «Chapple ILC, Mealey BL, Van Dyke TE, ym. Periodont...»127. Joissakin tapauksissa tavoitteeseen päästään vasta pidemmän ajanjakson kuluessa niin, että vuotoprosentti pienenee asteittain.
- Jos ienverenvuotoprosentti on > 30, potilas tarvitsee yksilöllisen tarpeen mukaista omahoidon motivointia ja ammattimaista hoitoa.
- Peri-implanttimukosiitin hoitovaste arvioidaan 2–3 kuukauden kuluttua «Herrera D, Berglundh T, Schwarz F, ym. Prevention ...»88.
- Terveessä peri-implanttikudoksessa ei esiinny verenvuotoa.
- Peri-implanttimukosiitin hoitovaste on riittävä, jos märkävuotoa ei todeta ja vuotopisteitä implantin ympärillä on korkeintaan yksi.
- Jos verenvuotoa esiintyy toistuvasti, potilas tarvitsee yksilöllisen tarpeen mukaista omahoidon motivointia ja ammattimaista hoitoa.
- Jos tavanomaisilla suuhygieniamenetelmillä ei saada toivottua vastetta, antimikrobisten suuvesien kuuriluontoisesta käytöstä saattaa joissain tapauksissa
olla hyötyä gingiviitin ja peri-implanttimukosiitin hoidossa omahoidon tukena.
- Päivittäinen purskuttelu klooriheksidiiniä, eteerisiä öljyjä tai setyylipyridiinikloridia sisältävällä suuvedellä ilmeisesti vähentää plakin määrää hampaiden pinnoilla ja gingiviittiä «Päivittäinen purskuttelu klooriheksidiiniä, eteerisiä öljyjä tai setyylipyridiinikloridia sisältävällä suuvedellä muun omahoidon tukena ilmeisesti vähentää plakin määrää hampaiden pinnoilla sekä ientulehdusta.»B.
- Klooriheksidiiniä voidaan käyttää erityisryhmissä (henkilöillä, jotka eivät muuten pysty huolehtimaan suuhygieniastaan) suun terveydenhuollon ammattihenkilön ohjeistuksen mukaan «al-Tannir MA, Goodman HS. A review of chlorhexidin...»166.
- On viitteitä siitä, että antimikrobisten suuvesien pitkäaikaiskäytöllä voi olla haitallisia paikallisia tai systeemisiä vaikutuksia, kuten syljen asetaldehydipitoisuuden suurentumista «Moazzez R, Thompson H, Palmer RM, ym. Effect of ri...»167, kserostomiaa «Chevalier M, Sakarovitch C, Precheur I, ym. Antise...»168 tai verenpaineen nousua «Bondonno CP, Liu AH, Croft KD, ym. Antibacterial m...»169.
- Tutkimustulokset alkoholipitoisten (yli 20-prosenttisten) suuvesien vaikutuksesta suusyövän suurentuneeseen riskiin ovat ristiriitaisia «Aceves Argemí R, González Navarro B, Ochoa García-...»170, «Ustrell-Borràs M, Traboulsi-Garet B, Gay-Escoda C....»171, «Carneiro CMM, Pinho PS, Teixeira JRB, ym. Unpaid d...»172.
Parodontiitin hoito
Vaiheen I–III parodontiitin hoito
- Tavoitteena on hoitaa infektio ja pysäyttää kudostuhon eteneminen sekä tasapainottaa mikrobiomin ja isännän vasteen välinen epätasapaino (eli dysbioosi).
- Tavoitteeseen päästään biofilmin mekaanisella poistolla ja inflammaation hallinnalla hammaslääkärin, suuhygienistin ja potilaan yhteistyönä.
- Taudin kulkuun ja riskitekijöihin puuttuminen jo ensimmäisten merkkien ilmaantuessa tuottaa hyvän ja usein pysyvän tuloksen ilman merkittäviä kudosvaurioita «Ramseier CA, Woelber JP, Kitzmann J, ym. Impact of...»173. Samalla se ehkäisee taudin vaikean muodon aiheuttamia toiminnallisia ja esteettisiä haittoja.
- Hoidon aluksi potilaalle kerrotaan parodontiitista, sen riskitekijöistä, vaikutuksista yleisterveyteen ja hoidosta. Yhteistyössä potilaan kanssa tehdään yksilöllinen hoitosuunnitelma, jota voidaan tarvittaessa muokata hoidon aikana.
- Potilasta opastetaan ja motivoidaan hyvään omahoitoon esimerkiksi motivoivan haastattelun
avulla «Motivoiva keskustelu saattaa olla tavanomaista omahoidon ohjausmenetelmää tehokkaampi ja saattaa parantaa sitä tehokkaammin suuhygieniatottumuksia, vähentää plakin määrää ja ienverenvuotoa.»C, «Werner H, Hakeberg M, Dahlström L, ym. Psychologic...»158, ks. myös lisätietoaineisto «Motivoiva haastattelu»6. Ks. videot motivoivasta haastattelusta «Videot: Motivoiva haastattelu»4. Omahoidon merkitystä ja potilaan omaa roolia parodontiitin hoidossa korostetaan
«Carra MC, Detzen L, Kitzmann J, ym. Promoting beha...»174.
- Yhdessä potilaan kanssa valitaan sopivat välineet hampaiden ja hammasvälien päivittäiseen puhdistamiseen huomioiden yksilölliset ongelmakohdat ja ohjataan niiden oikeaan käyttöön «Slot DE, Valkenburg C, Van der Weijden GAF. Mechan...»153.
- Hampaiden harjaukseen voidaan käyttää joko manuaalista hammasharjaa tai sähköhammasharjaa. Sähköhammasharjat poistavat tehokkaammin plakkia ja vähentävät enemmän gingiviittiä kuin manuaaliset hammasharjat «Sähköhammasharjat poistavat tehokkaammin plakkia ja vähentävät tehokkaammin ientulehdusta kuin tavalliset hammasharjat.»A.
- Hammasvälien koon perusteella valitaan sopivat välineet hammasvälien puhdistamiseen. Usein parodontiittipotilaille ensisijaisia ovat hammasväliharjat «Slot DE, Valkenburg C, Van der Weijden GAF. Mechan...»153. Harjatikun käyttö on osoittautunut hoitomyöntyvyyden kannalta helposti omaksuttavaksi, ja sen teho poistaa plakkia hammasväleistä on parempi kuin pelkän harjauksen «Sälzer S, Graetz C, Dörfer CE, ym. Contemporary pr...»150, «Worthington HV, MacDonald L, Poklepovic Pericic T,...»175. Hammaslanka soveltuu hammasvälien puhdistukseen, jos muu puhdistusväline ei mahdu hammasväliin «Chapple IL, Van der Weijden F, Doerfer C, ym. Prim...»176.
- Kotikäyttöisen, fotodynaamiseen kaksoisvaloterapiaan perustuvan laitteen vaikutuksesta ienverenvuodon, biofilmin määrän ja syventyneiden ientaskujen lukumäärän vähenemiseen parodontiittia sairastavien tavanomaisen omahoidon lisänä ei ole näyttöä pelkkään tavanomaiseen omahoitoon verrattuna «Kotikäyttöisen, fotodynaamiseen kaksoisvaloterapiaan perustuvan laitteen vaikutuksesta ienverenvuodon, biofilmin määrän ja syventyneiden ientaskujen lukumäärän vähenemiseen parodontiittia sairastavien tavanomaisen omahoidon lisänä ei ole näyttöä pelkkään tavanomaiseen omahoitoon verrattuna.»D.
- Toimiva omahoito on oleellisen tärkeää parodontiitin hoidon onnistumisen ja ennusteen kannalta. Omahoidon taso huomioidaan hoidon kaikissa vaiheissa ja tarvittaessa potilasta ohjataan ja motivoidaan tarkempaan omahoitoon «Van der Weijden FA, Slot DE. Efficacy of homecare ...»177.
- Hoidon alusta lähtien kiinnitetään huomiota parodontiitin riskitekijöihin «Ramseier CA, Woelber JP, Kitzmann J, ym. Impact of...»173.
- Motivoidaan potilasta tupakoinnin lopettamiseen ja korostetaan lopettamisen hyödyllisiä vaikutuksia «Tupakoinnin lopettaneilla ientaskut paranevat paremmin ja luukadon eteneminen hidastuu verrattuna tupakoitsijoihin.»A, ks. Käypä hoito -suositus Tupakka- ja nikotiiniriippuvuuden ehkäisy ja hoito «Tupakka- ja nikotiiniriippuvuuden ehkäisy ja hoito»6, «Tupakka- ja nikotiiniriippuvuuden ehkäisy ja hoito...»105 ja kyseisen suosituksen lisätietoartikkeli «Tupakka- ja nikotiinituotteista vieroitus suun terveydenhuollossa»7.
- Diabetesta sairastaville korostetaan hyvän hoitotasapainon merkitystä, ja ohjataan potilas tarvittaessa lääkärille «Tyypin 2 diabetes»8, «Tyypin 2 diabetes. Käypä hoito -suositus. Suomalai...»179.
- Profylaktista mikrobilääkitystä tarvitseville lääkitys annetaan ennen hoitotoimenpiteitä kansallisten suositusten mukaisesti. Ks. Käypä hoito -suositus Hammasperäiset äkilliset infektiot ja mikrobilääkkeet «Mikrobilääkkeet hammasperäisten infektioiden hoidossa ja komplikaatioiden ehkäisyssä»4, «Hammasperäiset äkilliset infektiot ja mikrobilääkk...»1 ja Husin endokardiittiprofylaksiohje «https://www.hus.fi/sites/default/files/2022-01/Endokardiittiprofylaksiohje.pdf»6.
- Parodontologiseen hoitoon sisältyy ammattimainen mekaaninen supra- ja subgingivaalisen plakin ja hammaskiven poisto sekä muiden plakkia retentoivien tekijöiden, kuten paikkaylimäärien, poisto «Suvan J, Leira Y, Moreno Sancho FM, ym. Subgingiva...»180, «Matalien (1–4 mm) ientaskujen hoidossa subgingivaalisella instrumentoinnilla saavutetaan paras hoitotulos. Keskisyvien (4–6 mm) ientaskujen hoidossa subgingivaalisella instrumentoinnilla saavutetaan yhtä hyvä hoitotulos kuin kirurgisella hoidolla.»A.
- Hoito voidaan tehdä joko ultraäänilaitteilla tai käsi-instrumenteilla. Molemmilla
päästään yhtä hyvään hoitotulokseen «Ultraäänilaitteilla ja käsi-instrumenteilla saadaan yhtä hyvä hoitotulos subgingivaalisessa instrumentoinnissa.»A.
- Subgingivaalisen instrumentoinnin ensisijaisena tavoitteena on dysbioottisen biofilmin hajotus ja poisto «Newman MG, Elangovan S, Dragan IF ym. Nonsurgical...»181.
- Hammaskiven ja plakkiretentioiden poistolla ja juurenpinnan kuntouksella luodaan biologisesti hyväksyttävä juuren pinta «Newman MG, Elangovan S, Dragan IF ym. Nonsurgical...»181.
- Tarvittaessa hoidossa käytetään pinta- tai paikallispuudutusta.
- Hoito voidaan tehdä koko hampaistoon 1–2 päivän aikana (full-mouth) tai useammalla
käyntikerralla sektoreittain (quadrant-wise). Molemmilla tavoilla päästään yhtä hyvään
hoitotulokseen «Parodontologinen instrumentointi voidaan tehdä lyhyen ajan sisällä koko suuhun tai pidemmällä aikavälillä osa-alueittain ja päästä samanlaiseen hoitotulokseen.»A.
- Systeeminen tulehdusreaktio on voimakkaampi silloin, kun hoito tehdään koko suuhun yhdellä kerralla, kuin silloin, kun hoito tehdään hampaistoneljännes kerrallaan «Jervøe-Storm PM, Eberhard J, Needleman I, ym. Full...»182, «Graziani F, Cei S, Orlandi M, ym. Acute-phase resp...»183.
- Subgingivaaliseen instrumentointiin liittyy joskus ohimenevää lämmönnousua ja huonovointisuutta «Jervøe-Storm PM, Eberhard J, Needleman I, ym. Full...»182.
- Omahoidon tukena voidaan tässä vaiheessa käyttää tapauskohtaisesti harkiten klooriheksidiinipurskuttelua kuuriluontoisesti «da Costa LFNP, Amaral CDSF, Barbirato DDS, ym. Chl...»184, «James P, Worthington HV, Parnell C, ym. Chlorhexid...»185.
- Parodontiittipotilaan tasapainoisesta purennasta on tärkeää huolehtia.
- Tarvittaessa puututaan purennan esikontakteihin osana ei-kirurgista hoitoa «Harrel SK, Nunn ME. The association of occlusal co...»69, esimerkiksi jos hampaassa on lisääntynyttä liikkuvuutta tai vertikaalisia luutaskuja.
- Sivuliikkeiden kulmahammasohjaus on tärkeää, ja joskus myös hampaiden muodon palauttaminen saattaa olla tarpeen.
- Systeemistä mikrobilääkitystä käytetään vain erityistapauksissa «Teughels W, Feres M, Oud V, ym. Adjunctive effect ...»186 kliinisen arvion ja mikrobiologisen näytteen perusteella. Ks. myös lisätietoaineisto
«Mikrobilääkitys»8.
- Kasvavan resistenssiongelman vuoksi mikrobilääkityksen tarvetta tulee harkita kriittisesti.
- Mikrobilääkitys voi tulla kyseeseen asianmukaiseen hoitoon huonosti vastaavan parodontiitin vaiheissa III–IV.
- Mikrobilääkitys aloitetaan tiiviisti aikataulutetun subgingivaalisen instrumentoinnin päätyttyä.
- Parodontologiseen hoitoon yhdistetty mikrobilääkitys saattaa vähentää kirurgian tarvetta «Mombelli A, Almaghlouth A, Cionca N, ym. Different...»187.
- Pieniannoksisen doksisykliinin (SDD) käyttöä ei suositella rutiinimaisesti parodontologisessa hoidossa «Sanz M, Herrera D, Kebschull M, ym. Treatment of s...»143, ja sen käyttö edellyttää hammaslääkäriltä asiaan perehtyneisyyttä «Donos N, Calciolari E, Brusselaers N, ym. The adju...»188.
- Hoidon eri vaiheissa huonoennusteisten hampaiden poistoa tulee harkita.
- Päätös hampaan poistosta tehdään aina potilaan tai hänen edustajansa kanssa.
- Hampaan poiston kynnystä madaltavat potilaan korkea ikä, riittämätön omahoito, runsas tupakointi, hampaan vähäinen merkitys purennan kokonaisuuden kannalta, hampaan huono kunto (esim. laaja kariesvaurio) ja potilaan sairaudet (esim. diabetes) «Helal O, Göstemeyer G, Krois J, ym. Predictors for...»189, «Chen X, Xu C, Wu Y, ym. The survival of periodonta...»190.
- Poistopäätöksessä voi olla apuna Dental Practicality Index (DPI) «Dawood A, Patel S. The Dental Practicality Index -...»191.
- Pitkälle edennyt furkaatiovaurio heikentää hampaan ennustetta. Asteen II tai III furkaatiovaurioisen hampaan poisto ei kuitenkaan ole ensisijainen hoitovaihtoehto, ks. alla kohta Erityiskysymyksiä «A2»3, «Dommisch H, Walter C, Dannewitz B, ym. Resective s...»192, «Jepsen S, Gennai S, Hirschfeld J, ym. Regenerative...»193.
Erityiskysymyksiä
- Vertikaalisten luutaskujen (joissa ientaskujen syvyys ≥ 6 mm ja luutaskujen syvyys ≥ 3 mm) hoitoon soveltuu usein regeneratiivinen läppäkirurgia edellyttäen, että ei-kirurginen hoitovaihe on tehty ensin ja omahoito on hyvää «Sanz M, Herrera D, Kebschull M, ym. Treatment of s...»143, «Nationella riktlinjer för tandvård. Stöd för styrn...»194. Läpän muotoiluun suositellaan kudosta säästävää niin sanottua minimaalisen avauksen läppätekniikkaa «Sanz M, Herrera D, Kebschull M, ym. Treatment of s...»143.
- Asteen II furkaatiovaurioiden hoitovaihtoehtoina voidaan harkita ei-kirurgista instrumentointia, läppäkirurgiaa, regeneratiivista kirurgiaa, premolarisaatiota (alamolaareissa) tai juurten radektomiaa.
- Asteen III furkaatiovaurioiden hoitovaihtoehtoina voidaan harkita ei-kirurgista instrumentointia, läppäkirurgiaa, tunnelointia, premolarisaatiota tai juurten radektomiaa.
- Tupakointi huonontaa vastetta parodontaalikirurgiaan ja regeneratiivisiin hoitomuotoihin ja voi vaikuttaa hoitomuodon valintaan «Patel RA, Wilson RF, Palmer RM. The effect of smok...»195.
- Hampaan kiinnityskudosten paranemisen seurauksena voi esiintyä ikenien vetäytymistä
ja vihlontaa paljastuneissa juurenpinnoissa «von Troil B, Needleman I, Sanz M. A systematic rev...»196.
- Potilaita ohjataan oikeaan harjaustekniikkaan, jolla pyritään ehkäisemään oireiden paheneminen. Heille kerrotaan, että happamat juomat ja ruoka-aineet pahentavat oireilua. Tarvittaessa käytetään vihloville hammaskauloille tarkoitettuja hammastahnoja, suuvesiä tai paikallisia desensitoivia aineita «Liu XX, Tenenbaum HC, Wilder RS, ym. Pathogenesis,...»197. Kovakudospuutokset voidaan hoitaa tarvittaessa soveltuvin menetelmin.
Vaiheen IV parodontiitin hoito
- Vaiheen IV parodontiitin hoito aloitetaan kuten vaiheen III. Lisäksi hoito voi sisältää
- purennan tasapainottamista ja hampaiden kiskottamisia «Dommisch H, Walter C, Difloe-Geisert JC, ym. Effic...»198.
- purennan kokonaisvaltaista arviointia ja hoitoa joko kiinteillä tai irrotettavilla proteeseilla «Carra MC, Rangé H, Swerts PJ, ym. Effectiveness of...»199, «Gotfredsen K, Rimborg S, Stavropoulos A. Efficacy ...»200, «Montero E, Molina A, Palombo D, ym. Efficacy and r...»201, «Herrera D, Sanz M, Kebschull M, ym. Treatment of s...»202
- hampaiden oikomishoitoa «Martin C, Celis B, Ambrosio N, ym. Effect of ortho...»203.
Hoitovasteen arviointi ja jatkohoidon suunnittelu
- Hoitovasteen arviointi tehdään 2–3 kuukauden kuluttua aktiivisen ei-kirurgisen hoidon päättymisen jälkeen. Suurin osa ientaskujen madaltumisesta tapahtuu 1–2 kuukauden kuluessa instrumentoinnista. Kliinisesti merkittävää ientaskujen madaltumista tapahtuu kuitenkin aina 6 kuukauteen asti «Paternò Holtzman L, Valente NA, Vittorini Orgeas G...»204.
- Käynnillä päivitetään esitiedot ja riskitekijät, arvioidaan omahoidon toteutuminen ja rekisteröidään parodontologinen status.
- Hoidon tavoitteena on, että koko suun ienverenvuotoprosentti on < 10, ei ole ≥ 4 mm:n
ientaskuja, joissa on verenvuotoa, eikä ≥ 6 mm:n ientaskuja «Siow DSF, Goh EXJ, Ong MMA, ym. Risk factors for t...»71, «Sanz M, Herrera D, Kebschull M, ym. Treatment of s...»143, «Suvan J, Leira Y, Moreno Sancho FM, ym. Subgingiva...»180, «Saydzai S, Buontempo Z, Patel P, ym. Comparison of...»205, «Sonnenschein SK, Betzler C, Rütters MA, ym. Long-t...»206, «Tomasi C, Leyland AH, Wennström JL. Factors influe...»207, «Rattu V, Raindi D, Antonoglou G, ym. Prevalence of...»208. Kaikkien hampaiden osalta hoidon päätepistettä ei välttämättä saavuteta heti ei-kirurgisen
hoidon päätteeksi etenkään vaikeassa ja pitkälle edenneessä parodontiitissa (vaiheet
III ja IV) «Rattu V, Raindi D, Antonoglou G, ym. Prevalence of...»208.
- Useat 5–6 mm:n ientaskut, furkaatiovauriot ja hammaskohtainen kiinnityskadon menetys ≥ 6 mm lisäävät parodontiitin etenemisen ja hampaan menettämisen todennäköisyyttä «Siow DSF, Goh EXJ, Ong MMA, ym. Risk factors for t...»71, «Rattu V, Raindi D, Antonoglou G, ym. Prevalence of...»208.
- Hampaiden menettämisen riski ei ole kuitenkaan merkittävästi suurentunut, jos hampaistossa on korkeintaan 4 kohtaa, joissa taskusyvyys on 5–6 mm «Rattu V, Raindi D, Antonoglou G, ym. Prevalence of...»208, «Feres M, Retamal-Valdes B, Faveri M, ym. Proposal ...»209.
- Hoitovasteen perusteella arvioidaan, tarvitseeko potilas jatkohoitoa vai siirtyykö
hän ylläpitohoitoon. Jatkohoito voi sisältää
- omahoidon tehostamisen
- toistetun instrumentoinnin «Toistetulla instrumentoinnilla saadaan ilmeisesti huomattava osa jäännöstaskuista paranemaan. Samalla kirurgian tarve ilmeisesti vähenee.»B
- mikrobinäytteen oton
- parodontaalikirurgiaa (ientaskusyvyydet ≥ 6 mm, furkaatiovaurioita, luutaskuja) «Sanz-Sánchez I, Montero E, Citterio F, ym. Efficac...»210.
- Kirurgian ehdottomia edellytyksiä ovat riittävä omahoito ja potilaan motivaatio.
- Jos kirurgialle ei ole edellytyksiä, toistetaan instrumentointi «Toistetulla instrumentoinnilla saadaan ilmeisesti huomattava osa jäännöstaskuista paranemaan. Samalla kirurgian tarve ilmeisesti vähenee.»B.
- Vaihtoehtoisia menetelmiä ovat näkökontrollin mahdollistava läppäkirurgia (access flap), resektiivinen ja regeneratiivinen kirurgia. Tupakointi huonontaa erityisesti regeneratiivisen kirurgian ennustetta.
- Jos omahoito ei ole riittävää, ei mikrobinäytteestä tai kirurgisista hoitomenetelmistä todennäköisesti ole hyötyä, vaan tällaisissa tilanteissa keskitytään ensisijaisesti omahoidon kohentamiseen ja toistettuun instrumentointiin.
- Omahoidon arvioimiseen voidaan käyttää koko suun ienverenvuotoprosenttia tai plakin määrää. Yli 20 %:n ienverenvuoto lisää parodontiitin etenemisen riskiä ja yli 30 %:n ienverenvuoto hampaiden menetyksen riskiä «Ramseier CA, Nydegger M, Walter C, ym. Time betwee...»211, «Matuliene G, Pjetursson BE, Salvi GE, ym. Influenc...»60.
- Ennen kirurgiaan siirtymistä instrumentointi voidaan toistaa useampia kertoja «Toistetulla instrumentoinnilla saadaan ilmeisesti huomattava osa jäännöstaskuista paranemaan. Samalla kirurgian tarve ilmeisesti vähenee.»B, «Sanz-Sánchez I, Montero E, Citterio F, ym. Efficac...»210.
Peri-implantiitin hoito
- Hoidon ensisijaisena tavoitteena on hoitaa infektio ja pysäyttää kudostuhon eteneminen.
- Ei-kirurgisen hoidon tavoitteena on biofilmin mekaaninen poisto ja inflammaation hallinta.
- Hoito aloitetaan aina ei-kirurgisella hoidolla, ja jos sillä ei saavuteta toivottua tulosta, harkitaan kirurgista hoitoa.
- Hoito perustuu myös riskitekijöiden hallintaan (taulukko «Peri-implanttisairauksille altistavia ja syytekijöitä ...»2).
- Ei-kirurgisen peri-implantiitin hoidon vaiheet ovat «Cosgarea R, Roccuzzo A, Jepsen K, ym. Efficacy of ...»212, «de Waal YCM, Winning L, Stavropoulos A, ym. Effica...»213, «Liñares A, Sanz-Sánchez I, Dopico J, ym. Efficacy ...»214
- omahoidon ohjaus
- riskitekijöihin puuttuminen
- proteettisten rakenteiden irrotus/puhdistus/muokkaus huomioiden puhdistettavuus sekä plakkiretentiivisyys
- biofilmin poisto käyttäen soveltuvia instrumentteja (titaani-instrumentit sekä implanttien puhdistukseen soveltuvat ultraäänikärjet, jauhepuhdistimet tai harjat ja kumikupit)
- mikrobilääkkeiden käyttöä ei rutiinimaisesti suositella, mutta sitä voidaan tapauskohtaisesti harkita strategisesti tärkeissä hyväennusteisissa implanteissa, joissa on syviä (≥ 7 mm tai syvempiä) taskuja ja runsasta märkävuotoa «Herrera D, Berglundh T, Schwarz F, ym. Prevention ...»88.
- Hoitovasteen arviointi suositellaan tehtäväksi 2–3 kuukauden päästä hoidosta, ja hoitovasteesta riippuen edetään joko ylläpitohoitoon tai kirurgiseen hoitoon «Herrera D, Berglundh T, Schwarz F, ym. Prevention ...»88.
- Hoitovasteen arvioinnissa tulee huomioida verenvuoto tai märkävuoto taskumittauksen yhteydessä
sekä taskusyvyys:
- Jos taskusyvyydet ovat 5 mm tai alle eikä taskumittauksen yhteydessä esiinny verenvuotoa tai märkävuotoa, potilaan voi siirtää ylläpitohoitoon.
- Jos taskusyvyydet ovat > 5 mm ja mittauksen yhteydessä esiintyy verenvuotoa useammalta kuin yhdeltä pinnalta tai esiintyy märkävuotoa ja todetaan etenevää luukatoa alkutilanteeseen nähden, suositellaan siirtymistä kirurgiseen hoitoon «Cosgarea R, Roccuzzo A, Jepsen K, ym. Efficacy of ...»212, «de Waal YCM, Winning L, Stavropoulos A, ym. Effica...»213, «Liñares A, Sanz-Sánchez I, Dopico J, ym. Efficacy ...»214, «Herrera D, Berglundh T, Schwarz F, ym. Prevention ...»88.
- Hoidon eri vaiheissa huonoennusteisten implanttien päällysrakenteiden tai koko implantin poistoa tulee harkita.
Ylläpitohoito
- Kun riittävän hyvä hoitotulos on saavutettu, potilas siirtyy ylläpitohoitoon, joka
toteutetaan yksilöllisen hoitovälin mukaisesti 3–12 kuukauden välein «Ramseier CA, Nydegger M, Walter C, ym. Time betwee...»211.
- Ylläpitohoitoväli määritetään saavutetun hoitotuloksen ja riskitekijöiden perusteella «Parodontiitin etenemisen riskiä ylläpitohoidossa olevilla potilailla voidaan ennakoida PRA-riskinarviointimallin avulla.»A. Kliinikon tueksi näiden määrittämiseen on saatavilla yksilöllinen riskikartoitusmalli «https://www.perio-tools.com/pra/en/»7 sekä ylläpitohoitovälin määritykseen suunniteltu työkalu «https://www.perio-tools.com/spt/uk/»8.
- Ylläpitohoidon seuraava ajankohta arvioidaan jokaisella ylläpitohoitokäynnillä, ja se voi vaihdella samalla potilaallakin kliinisen tilanteen ja riskitekijöiden muutoksien mukaan.
- Riskitekijät huonontavat hoitotulosta etenkin yhtäaikaisesti esiintyessään, eikä säännöllisellä ylläpitohoidollakaan välttämättä pystytä pysäyttämään parodontiitin etenemistä.
- Kun peri-implantiitti on hoidettu, ylläpitohoitoa suositellaan 3–4 kuukauden välein ensimmäisen vuoden ajan. Tämän jälkeen määritetään yksilöllinen ylläpitohoitoväli. Parhaaseen tulokseen päästään, kun ylläpitohoitoväli on enintään 6 kuukautta «Herrera D, Berglundh T, Schwarz F, ym. Prevention ...»88, «Monje A, Aranda L, Diaz KT, ym. Impact of Maintena...»163. Kliinikon tukena riskitekijöiden kartoittamiseen voidaan käyttää IDRA-työkalua «https://www.perio-tools.com/idra/en/»2.
- Ylläpitohoitokäynneillä päivitetään esitiedot ja riskitekijät, rekisteröidään parodontologinen status ja tehdään supra- ja subgingivaalinen ammattimainen puhdistus. Riittävästä fluoriprofylaksista huolehditaan, etenkin jos potilaalla on kariesriskitekijöitä tai paljastuneita hammaskauloja. Omahoidon toteutuminen arvioidaan ja potilasta ohjataan ja motivoidaan tarvittaessa tarkempaan omahoitoon «Slot DE, Valkenburg C, Van der Weijden GAF. Mechan...»153. Ks. videot motivoivasta haastattelusta «Videot: Motivoiva haastattelu»4.
- Ylläpitohoito voidaan tehdä käsi-instrumenteilla, ultraäänilaitteella tai jauhepuhdistimella
«Jauhepuhdistus on tehokas ja kivuton menetelmä jäännöstaskujen ylläpitohoidossa.»B.
- Jauhepuhdistimella ei voida poistaa hammaskiveä.
- Antimikrobisten suuvesien kuuriluonteisesta käytöstä saattaa joissakin tapauksissa olla hyötyä omahoidon tukena. Klooriheksidiiniä, eteerisiä öljyjä tai setyylipyridiinikloridia sisältävien suuvesien käyttö ilmeisesti vähentää plakin määrää hampaiden pinnoilla ja gingiviittiä «Päivittäinen purskuttelu klooriheksidiiniä, eteerisiä öljyjä tai setyylipyridiinikloridia sisältävällä suuvedellä muun omahoidon tukena ilmeisesti vähentää plakin määrää hampaiden pinnoilla sekä ientulehdusta.»B.
- Säännöllinen ylläpitohoito vähentää sekä pitkällä että lyhyellä aikavälillä kiinnityskatoa ja hampaiden sekä implanttien menetystä «Trombelli L, Franceschetti G, Farina R. Effect of ...»215, «Monje A, Aranda L, Diaz KT, ym. Impact of Maintena...»163, «Parodontiitin etenemistä ja hampaiden menetystä ylläpitohoidon aikana ennustavat potilaan tupakointi, epäsäännöllinen ylläpitohoidossa käynti, parodontiitin vaikeusaste alkutilanteessa ja jäännöstaskujen määrä ylläpitohoidon aikana.»A, «Smoking, irregular supportive periodontal treatment (maintenance) and presence of periodontitis or periodontitis with poor response to treatment are significant risk factors for peri-implantitis and implant loss.»A.
- Jos todetaan merkkejä taudin uusiutumisesta, varataan erillinen hoitoaika.
- Taudin uusiutumiseen vaikuttavat samat riskitekijät kuin taudin syntyyn (taulukko «Parodontiitille ja sen uusiutumiselle altistavia ja syytekijöitä...»1).
Parodontiumin akuutit infektiot (parodontaaliset absessit)
- Parodontiumin akuuttien infektioiden (parodontaalisten absessien) esiintyvyys on 8–14 % kaikista suun äkillisistä infektioista. Hoitamattomaan parodontiittiin liittyvien absessien esiintyvyys on yli nelinkertainen verrattuna hoidettujen potilaiden parodontiitin akutisoitumisiin «Herrera D, Retamal-Valdes B, Alonso B, ym. Acute p...»216.
- Potilaat hakeutuvat parodontaalisten absessien vuoksi päivystykseen, ja ne vaativat välitöntä diagnosointia ja hoitoa.
- Parodontiumin äkillisissä infektioissa kudostuho etenee usein nopeasti ja voi huonontaa hampaan ennustetta huomattavasti, erityisesti jos potilaalla on vaikea tai pitkälle edennyt parodontiitti (vaiheet III ja IV). Lisäksi akuutteihin parodontiumin infektioihin voi liittyä systeemisiä riskejä «Herrera D, Retamal-Valdes B, Alonso B, ym. Acute p...»216.
- Parodontiumin alueelle kehittyvän absessin etiologiana voi olla myös muita syitä kuin parodontiitti (ks. lisätietoaineisto Parodontaalisten absessien luokittelu «Parodontaalisten absessien luokittelu»9).
Parodontiittiin liittyvä absessi
- Parodontiittiin liittyvässä absessissa on kyseessä parodontiitin äkillinen paheneminen, ja se voi liittyä hoitamattomaan parodontiittiin tai sairauden eri hoitovaiheisiin.
- Parodontiittiin liittymättömissä tiloissa aiheuttajana voi olla muun muassa vierasesine, tavat, purenta, ikenen liikakasvu tai juurenpinnan poikkeamat (ks. lisätietoaineisto Parodontaalisten absessien luokittelu «Parodontaalisten absessien luokittelu»9).
Kehittyminen ja oireet
- Ientaskun mikrobiston epätasapaino laukaisee ienkudoksen tulehdusvasteen, joka on
akuutissa vaiheessa voimakas.
- Absessi kehittyy taskuseinän pehmytkudoksen sisälle, josta se voi levitä parodontaaliligamenttiin ja alveoliluuhun.
- Kliinisesti todetaan ientaskun seinämän turvotus ja ienverenvuoto «Herrera D, Retamal-Valdes B, Alonso B, ym. Acute p...»216, «Papapanou PN, Sanz M, Buduneli N, ym. Periodontiti...»129
- Absessiin voi liittyä paikallisia oireita ja muita kliinisiä löydöksiä, kuten äkillinen, usein voimakas kipu, turvotus ja nopeasti edennyt kudostuho, märkävuoto, puruarkuus, hampaan lisääntynyt liikkuvuus ja hampaan siirtyminen alveolikuopassa «Herrera D, Retamal-Valdes B, Alonso B, ym. Acute p...»216, «Papapanou PN, Sanz M, Buduneli N, ym. Periodontiti...»129.
- Systeemiset oireet ja löydökset, kuten lämmönnousu, paikallisten imusolmukkeiden turvotus, valkosolujen määrän suureneminen, pahoinvointi ja ekstraoraalinen turvotus, ovat mahdollisia «Herrera D, Retamal-Valdes B, Alonso B, ym. Acute p...»216, «Papapanou PN, Sanz M, Buduneli N, ym. Periodontiti...»129, «Herrera D, Roldán S, González I, ym. The periodont...»217.
Diagnoosit
- Parodontiittiin liittyvä absessi tulee diagnoosiksi, kun todetaan ientaskun seinämän
turvotus ja ienverenvuoto, jotka liittyvät parodontiittiin «Herrera D, Retamal-Valdes B, Alonso B, ym. Acute p...»216, «Papapanou PN, Sanz M, Buduneli N, ym. Periodontiti...»129.
- Yksinkertaisessa absessissa märkä purkautuu joko ientaskun seinämän kautta ientaskuun (K05.20) tai ikenen pehmytkudoksen läpi suoraan suuonteloon, jolloin syntyy näkyvä fisteli (K05.21).
- Kompleksissa absessissa infektio leviää luun tai hampaan lateraaliseinämän kautta esimerkiksi vastakkaiselle puolelle hammasta ja purkautuu sieltä joko ientaskuun (K05.20) tai fistelin kautta suoraan suuonteloon (K05.21).
- Hoitamattomana absessi voi kroonistua joko ilman fisteliä tai fistelin kanssa (K05.31).
Erotusdiagnostiikka
- Erotusdiagnostiikassa tulee ottaa huomioon parodontiumin alueelle muista syistä kuin parodontiitista kehittyvät absessit «Herrera D, Feres M. Treatment of acute periodontal...»218. Ks. taulukko «Parodontaalisen absessin ja endo-paroleesion erotusdiagnostisia merkkejä ....»6 (ks. myös lisätietoaineisto Parodontaalisten absessien luokittelu «Parodontaalisten absessien luokittelu»9).
- Tällaisia ovat esimerkiksi
- dentoalveolaariset absessit (ks. Käypä hoito -suositus Hammasperäiset äkilliset infektiot ja mikrobilääkkeet «Mikrobilääkkeet hammasperäisten infektioiden hoidossa ja komplikaatioiden ehkäisyssä»4, «Hammasperäiset äkilliset infektiot ja mikrobilääkk...»1), perikoroniitti (ks. Käypä hoito -suositus Viisaudenhammas «Viisaudenhammas»5, «Viisaudenhammas. Käypä hoito -suositus. Suomalaise...»101), periapikaalinen absessi ja endo-paroleesiot (ks. Käypä hoito -suositus Hampaan juurihoito «Hampaan juurihoito»9, «Hampaan juurihoito. Käypä hoito -suositus. Suomala...»219)
- lateraalinen periapikaalinen kysta, vertikaaliset juurimurtumat ja postoperatiiviset absessit.
- Erotusdiagnostisia tutkimuksia ovat muun muassa pulpan herkkyystesti ja röntgenkuvaus (esim. fistulografia).
| Parodontaaliseen absessiin viittaavat | Endodonttiseen alkuperään viittaavat |
|---|---|
|
|
- Erotusdiagnostiikassa on tärkeää huomioida myös muiden harvinaisten suuontelossa esiintyvien
parodontaalista absessia muistuttavien leesioiden mahdollisuus. Tällaisia ovat esimerkiksi:
- levyepiteelisyövät, muut kasvaimet ja kasvainten etäpesäkkeet
- pyogeeninen granulooma, perifeerinen luutuva fibrooma, odontogeeninen keratokysta, eosinofillinen granulooma
- itse aiheutetut vauriot.
- Harkinnan mukaan otetaan kudosnäyte histopatologista diagnoosia varten.
Hoito
- Mikäli absessi ei liity parodontiittiin, kohdistetaan hoito syyn mukaisesti «Parodontaalisten absessien luokittelu»9.
- Parodontiittiin liittyvän absessin hoito koostuu kahdesta eri vaiheesta: 1) akuutin
vaiheen hoito, jonka tavoite on pysäyttää kudostuho ja pitää oireet hallinnassa ja
2) absessia edeltäneen tilan tai jäännösleesion hoito.
- Akuutissa vaiheessa
- ientaskun suuta raotetaan joko ientaskumittarilla tai käsi-instrumentilla, jotta märkä pääsee purkautumaan
- märkäkeräymän poistumista voidaan edesauttaa kevyesti painamalla pehmytkudosta koronaalisuuntaan välttäen voimakasta kudosmanipulaatiota
- kompleksin absessin kanavointi taskunsuun kautta ei ole aina mahdollista ja absessiin voidaan tehdä insisio sen korkeimman kohouman kohdalta terävällä instrumentilla
- jos leesio on hyvin saavutettavissa, juuren pinnalta poistetaan kovat ja pehmeät bakteeripeitteet
- instrumentointiin ja biofilmin rikkomiseen soveltuvat ikenenalaiseen työskentelyyn tarkoitetut sirot ultraäänikärjet ja pitkäkaulaiset mini-/mikrokyretit
- akuutissa vaiheessa pehmytkudosten kaapimista (kyretointia) tulee välttää, koska se voi johtaa paranemisvaiheeseen tarvittavien kudoskomponenttien menetykseen ja heikentää kiinnityskudosten regeneraatiota «Herrera D, Feres M. Treatment of acute periodontal...»218
- erityisesti papillat pyritään säilyttämään koskemattomina
- voimakasta taskun huuhtelua puhdistuksen jälkeen vältetään, koska tavoitteena on saada hyvä, stabiili verihyytymä taskualueelle
- mahdollisimman minimaalinen ja hellävarainen instrumentointi vähentää hoidon jälkeistä oireilua ja ikenen vetäytymistä ja lyhentää paranemisaikaa «Nibali L, Pometti D, Chen TT, ym. Minimally invasi...»220, «Kučič AC, Gašperšič R. Minimally invasive non-surg...»221, «Ng E, Tay JRH, Ong MMA. Minimally Invasive Periodo...»222, «Ribeiro FV, Mehta JJ, Monteiro MF, ym. Minimal inv...»223. Tulokset ovat hyvät myös pitkässä seurannassa (5 vuotta) «Nibali L, Yeh YC, Pometti D, ym. Long-term stabili...»224.
- kirurgista hoitoa ei tulisi tehdä hoidon alkuvaiheessa «Ng E, Tay JRH, Ong MMA. Minimally Invasive Periodo...»222
- Jos hampaaseen kohdistuu traumaattinen purentapaine, kevennetään purentarasitusta.
- Jos hampaassa on merkittävää horisontaalista liikkuvuutta tai hammas on epäedullisessa asennossa purentavoimaan nähden, se voidaan tarvittaessa vakauttaa väliaikaisesti esimerkiksi kiskottamalla.
- Yleisterveen potilaan yksinkertaisen absessin hoidossa ei mikrobilääkitys yleensä ole tarpeellinen, ellei potilaalla ole yleisoireita.
- Kompleksissa absessissa mikrobilääkitys voi olla aiheellinen infektion leviämisen estämiseksi, vaikkei yleisoireita olisikaan. Mikrobilääkevalinnasta ks. Käypä hoito -suositus Hammasperäiset äkilliset infektiot ja mikrobilääkkeet «Mikrobilääkkeet hammasperäisten infektioiden hoidossa ja komplikaatioiden ehkäisyssä»4, «Hammasperäiset äkilliset infektiot ja mikrobilääkk...»1.
- Jos potilaalla on suurentunut infektioriski, paranemista komplisoiva sairaus tai lääkitys, mikrobilääkehoidon kynnys on matalampi kuin yleisterveen potilaan hoidossa (ks. Käypä hoito -suositus Hammasperäiset äkilliset infektiot ja mikrobilääkkeet «Mikrobilääkkeet hammasperäisten infektioiden hoidossa ja komplikaatioiden ehkäisyssä»4, «Hammasperäiset äkilliset infektiot ja mikrobilääkk...»1).
- Akuutissa vaiheessa
- Vaste akuutin vaiheen hoitoon tarkastetaan viimeistään 3 vuorokauden päästä. Tällöin
- selvitetään, onko absessi rauhoittunut ja ovatko oireet vaimenneet
- arvioidaan, onko mikrobilääkityksen tai muun lisähoidon tarvetta, ja sovitaan paranemisen jälkitarkastus 2–3 kuukauden päähän, jolloin tehdään kokonaishoidon tarvearvio ja jatkohoitosuunnitelma.
Endo-paroleesio
- Endo-paroleesiolla (EPL) tarkoitetaan tilannetta, jossa hammaspulpa ja marginaalinen parodontium ovat infektoituneet.
Kehittyminen ja oireet
- Endo-paroleesio voi saada alkunsa pulpan, parodontiumin tai näiden molempien infektiosta
«Herrera D, Retamal-Valdes B, Alonso B, ym. Acute p...»216.
- Kyseessä on yleensä krooninen tila, jonka akutisoituessa siihen voi liittyä absessi.
- Tilaan liittyy aina jonkinlainen juuriontelon ja parodontiumin kudosten infektion ja inflammaation yhdistyminen.
- Leesion etiologiana voi myös olla juuren tai furkaation perforaatio, juuren fraktuura, resorptio tai trauman jälkeinen pulpan nekroosi «Herrera D, Retamal-Valdes B, Alonso B, ym. Acute p...»216, ks. lisätietoaineisto Endo-paroleesioiden luokittelu «Endo-paroleesioiden luokittelu»10.
Hoito
- Hoidon alussa voi olla vaikeaa selvittää, onko kyseessä endo-paroleesio vai pelkästään parodontiittiin liittyvä tila (taulukko «Parodontaalisen absessin ja endo-paroleesion erotusdiagnostisia merkkejä ....»6).
- Jos todetaan parodontaalista alkuperää oleva tilanne, jossa hammas on vitaali, hoito
noudattaa parodontiittiin liittyvän absessin hoitoperiaatteita.
- Jos parodontaalista alkuperää olevan tilan seurauksena todetaan juurikanavainfektio, aloitetaan hoito juurihoidolla ja tehdään samanaikaisesti subgingivaalinen hoito parodontiittiin liittyvän absessin hoitoperiaatteiden mukaisesti.
- Tarvittaessa jatketaan parodontologista hoitoa 2–3 kuukauden kuluttua, kun periapikaalinen leesio on parantunut.
- Jos todetaan devitaali juurikanava, hoito aloitetaan juurihoidolla, ks. Käypä hoito
-suositus Hampaan juurihoito «Hampaan juurihoito»9, «Hampaan juurihoito. Käypä hoito -suositus. Suomala...»219.
- Jos endo-paroleesion alkuperänä on juurikanavan infektion purkautuminen ientaskun kautta, juurihoitoon saadaan yleensä positiivinen vaste varsin nopeasti, hoidon ennuste on yleensä hyvä eikä muuta hoitoa tarvita.
- Jos kyseessä on juurikanavainfektion ja parodontiumista peräisin olevan infektion
yhdistyminen, parodontaalileesio ei parane pelkällä juurihoidolla.
- Tällöin tehdään hampaan hoidettavuusarvio (ks. Käypä hoito -suosituksen Hampaan juurihoito lisätietoaineisto «Hampaan hoidettavuus suhteessa viereisiin hampaisiin sekä suun- ja yleisterveyteen, Dental Practicality Index (DPI)»11). Jos hammas päätetään säilyttää, tehdään juurikanavien kemomekaaninen puhdistus ja parodontologinen subgingivaalinen hoito samanaikaisesti «Herrera D, Feres M. Treatment of acute periodontal...»218 parodontaalisen absessin hoitoperiaatteiden mukaisesti.
- Parodontaalivaurion laajuus vaikuttaa hoidon ennusteeseen: parodontiitin vaiheissa I ja II vaikutus ennusteeseen on vähäinen, mutta parodontiitin vaiheissa III ja IV leesion laajuuden suurentuessa ennuste heikkenee (ks. lisätietoaineisto Endo-paroleesioiden luokittelu «Endo-paroleesioiden luokittelu»10).
- Jos kyseessä ovat erilliset leesiot, parodontologinen ja endodonttinen hoito voidaan tehdä samanaikaisesti. Aikaviive hoitojen välillä ei vaikuta ratkaisevasti ei-kirurgisten hoitoprosessien jälkeiseen paranemiseen «Gupta S, Tewari S, Tewari S, ym. Effect of Time La...»225.
- Tapauskohtaisesti voidaan harkita sekä parodontologista että endodonttista regeneratiivista kirurgiaa jatkohoitona, mikäli muut edellytykset täyttyvät eikä vasta-aiheita ole «Cortellini P, Stalpers G, Mollo A, ym. Periodontal...»226, «AlJasser R, Bukhary S, AlSarhan M, ym. Regenerativ...»227.
- Laajan endo-paroleesion ennustetta huonontavat tupakointi, syvät ientaskut, kiinnityskadon määrä, koko suun parodontiitin vaikeusaste ja hampaan juurikanavien lukumäärä «Fan X, Xu X, Yu S, ym. Prognostic Factors of Grade...»228.
Tiimityö parodontologisessa hoidossa
- Potilaan ja hammaslääkärin ohella parodontologisen hoitotiimin jäseniä voivat olla suuhygienisti, hammashoitaja ja erikoishammaslääkäri. Ks. kaavio «hoi50086d.pdf»4.
- Potilaan omahoito ja sitoutuminen hoitoon ovat parodontologisen hoidon onnistumisen edellytys. Joissakin tapauksissa (esim. hoivan varassa olevan potilaan) omainen tai hoitohenkilökunta avustaa omahoidossa.
- Hammaslääkäri tekee parodontologisen diagnoosin ja laatii sen perusteella hoitosuunnitelman.
- Hammaslääkäri osallistuu hoitoon ja vastaa aina sen toteutumisesta kokonaisuutena.
- Suuhygienisti huolehtii osaltaan suun terveyden ylläpitämisestä, tekee hoidon tarpeen arvioita ja terveystarkastuksia ja osallistuu hoitoon ja ylläpitohoitoon.
- Jos tarvittavat hoitotoimenpiteet ylittävät oman osaamisen, potilas on ohjattava jatkohoitoon.
- Säännöllisestä ylläpitohoidosta huolimatta etenevä tai uusiutuva parodontiitti (10–20 %:lla potilaista) edellyttää erikoishammaslääkäritasoista hoitoa «Pastagia J, Nicoara P, Robertson PB. The effect of...»229.
- Potilas voidaan lähettää harkinnan mukaan parodontologiseen hoitoon perehtyneelle
(erikois-)hammaslääkärille esimerkiksi, kun kyseessä on
- vaiheen III–IV parodontiitti, jossa toimenpiteet ovat erittäin vaativia (syvät taskut, furkaatiovauriot, vaikeapääsyiset pinnat)
- parodontiitti, jossa purenta tai endodonttiset ongelmat ovat osana etiologiaa
- vaikea tai pitkälle edennyt parodontiitti, joka liittyy pitkäaikaissairauteen
- vaikea nuoruusiän parodontiitti
- vaativaa parodontaalikirurgista hoitoa tarvitseva potilas
- peri-implantiitin kirurginen hoito
- tilanne, jossa asianmukaisen hoidon jälkeen on merkkejä aktiivisesta sairaudesta.
- Ks. myös kaavio parodontologisesta hoitopolusta ja työnjaosta «hoi50086d.pdf»4.
Potilasnäkökulma
- Parodontiitti huonontaa elämänlaatua, ja elämänlaadun heikkeneminen on yhteydessä parodontiitin vaikeusasteeseen ja hammaspuutoksiin «Paśnik-Chwalik B, Konopka T. Impact of periodontit...»230. Elämänlaatua huonontavat sairauden aiheuttama kipu sekä toiminnalliset, sosiaaliset ja psyykkiset ongelmat.
- Potilaiden kokemusten mukaan omahoitoa
- edistävät konkreettinen suunnitelma päivittäisen omahoidon toteuttamiseksi, mahdollisuus arvioida omahoitoa itse esimerkiksi plakkivärin avulla, ymmärrettävän tutkimustiedon saaminen ja suunhoitotuotteiden hyvä saatavuus
- estävät ristiriitainen tieto, epäselvät tavoitteet, suunhoitotuotteiden kustannukset, ympäristö, joka ei tue omahoidon pyrkimyksiä, hammashoitopelko ja kivun pelko «Raval P, Moreno F, Needleman I. Patient involvemen...»231.
- Parodontiitin hoito näyttäisi parantavan suun terveyteen liittyvää elämänlaatua «Mendez M, Melchiors Angst PD, Stadler AF, ym. Impa...»232, «Rawlinson A, Vettore MV, Baker SR, ym. Periodontal...»233.
Parodontiitin yhteys pitkäaikaissairauksiin ja yleisterveyteen
- Hampaan kiinnityskudosten sairaudet vaikuttavat yleisterveyteen.
- Parodontiitti ilmeisesti lisää ja pitää hoitamattomana yllä elimistön lievää tulehdustilaa «Paraskevas S, Huizinga JD, Loos BG. A systematic r...»234.
- Parodontiittia sairastavilla on ilmeisesti suurentunut
- sydän- ja verisuonitautien, kuten sepelvaltimotaudin ja aivoinfarktin, riski «Parodontiittipotilailla ilmeisesti esiintyy enemmän sydän- ja verisuonitauteja, kuten sepelvaltimotautia ja aivoinfarkteja, kuin parodontaalisesti terveillä.»B
- diabeteksen hoitotasapainon huonontumisen ja komplikaatioiden riski «Lalla E, Papapanou PN. Diabetes mellitus and perio...»235, «Preshaw PM, Alba AL, Herrera D, ym. Periodontitis ...»236, «Sanz M, Ceriello A, Buysschaert M, ym. Scientific ...»237.
- Parodontiittia sairastavilla saattaa olla suurentunut
- raskauskomplikaatioiden, kuten ennenaikaisen synnytyksen, lapsen pienen syntymäpainon ja pre-eklampsian (raskaudenaikainen monielinsairaus, jossa verenpaine nousee 20. raskausviikon jälkeen ja ilmaantuu proteinuriaa tai löydöksiä muista elinjärjestelmistä) «Pre-eklampsia - tutkimustiedosta kotimaiseen hoito...»238, riski «Raskaana olevilla parodontiittipotilailla saattaa esiintyä enemmän raskauskomplikaatioita, kuten ennenaikaista synnytystä, lapsen pientä syntymäpainoa ja pre-eklampsiaa, kuin raskaana olevilla, jotka eivät sairasta parodontiittia.»C
- hengityselinsairauksien, kuten keuhkoahtaumataudin, uniapnean ja vakavan COVID-19:n, riski «Parodontiittia sairastavilla saattaa esiintyä enemmän hengityselinsairauksia, kuten keuhkoahtaumatautia, obstruktiivista uniapneaa ja vakavaa COVID-19:ää, kuin parodontaalisesti terveillä.»C
- nivelreuman riski «Qiao Y, Wang Z, Li Y, ym. Rheumatoid arthritis ris...»239.
- Huono suun terveys saattaa suurentaa laitos- ja sairaalapotilaiden riskiä sairastua
pneumoniaan «Huono suuhygienia saattaa lisätä keuhkokuumeen esiintymistä laitos- ja sairaalapotilailla. Suuhygienian parantamisella saatetaan voida ehkäistä keuhkokuumeen kehittymistä näillä potilailla.»C.
- Suuhygienian parantamisella saatetaan voida ehkäistä laitos- ja sairaalapotilaiden pneumonioita «Huono suuhygienia saattaa lisätä keuhkokuumeen esiintymistä laitos- ja sairaalapotilailla. Suuhygienian parantamisella saatetaan voida ehkäistä keuhkokuumeen kehittymistä näillä potilailla.»C.
- Parodontiitin hoito ilmeisesti
- lieventää elimistön lievää tulehdustilaa «Paraskevas S, Huizinga JD, Loos BG. A systematic r...»234, «D'Aiuto F, Orlandi M, Gunsolley JC. Evidence that ...»240, «Teeuw WJ, Slot DE, Susanto H, ym. Treatment of per...»241, «Artese HP, Foz AM, Rabelo Mde S, ym. Periodontal t...»242, «Luthra S, Orlandi M, Hussain SB, ym. Treatment of ...»243
- parantaa tyypin 2 diabetesta sairastavan glukoositasapainoa «Parodontiittia ja tyypin 2 diabetesta sairastavien potilaiden parodontiitin hoito ilmeisesti parantaa diabeteksen hoitotasapainoa (interventioryhmässä HbA1c-arvo pieneni keskimäärin 0,4 % enemmän kuin verrokkiryhmässä).»B
- vaikuttaa edullisesti sydän- ja verisuonitautiriskiin liittyviin tekijöihin, muun muassa seerumin CRP-, IL-6-, TNF-alfa- ja fibrinogeenipitoisuuteen «Teeuw WJ, Slot DE, Susanto H, ym. Treatment of per...»241, «Esteves Lima RP, Atanazio ARS, Costa FO, ym. Impac...»244, «Shah B, Shah M, Geisinger M, ym. Effect of non-sur...»245
- parantaa endoteelifunktiota «Teeuw WJ, Slot DE, Susanto H, ym. Treatment of per...»241.
- Parodontologinen hoito saattaa pienentää nivelreuman tautiaktiivisuutta «Sun J, Zheng Y, Bian X, ym. Non-surgical periodont...»246.
- Raskaudenaikaisella parodontologisella hoidolla ei liene vaikutusta raskauskomplikaatioiden ehkäisyssä «Gingiviittiä tai parodontiittia sairastavien raskaudenaikaisella parodontologisella hoidolla ei liene vaikutusta raskauskomplikaatioiden esiintymiseen verrattuna hoitamattomuuteen.»C.
- Parodontologisen hoidon vaikuttavuudesta sydän- ja verisuonitautien «Parodontologisen hoidon vaikutuksesta sydän- ja verisuonitautien primaari- tai sekundaariehkäisyssä ei ole näyttöä.»D ja hengityselinsairauksien ehkäisyssä ei ole näyttöä «Molina A, Huck O, Herrera D, ym. The association b...»247.
Kustannusasiat
- Parodontologinen hoito on kustannustehokasta «Parodontiitin ammattimainen hoito aiheuttaa potilaalle kustannuksia, mutta se on kuitenkin ilmeisesti edullisempaa kuin useiden menetettyjen hampaiden korvaaminen joko kiinteillä silloilla tai hammasimplantein.»B, «Fardal Ø, Grytten J. Applying quality assurance in...»248, «Martin JA, Fardal Ø, Page RC, ym. Incorporating se...»249, «Schwendicke F, Plaumann A, Stolpe M, ym. Retention...»250, «Schwendicke F, Graetz C, Stolpe M, ym. Retaining o...»251, «Nagpal D, Ibraimova L, Ohinmaa A, ym. The cost-eff...»252, «Schwendicke F, Stolpe M, Plaumann A, ym. Cost-effe...»253.
- Ehkäisevällä ja varhaisella parodontologisella hoidolla voidaan vähentää hammashoidon kokonaistarvetta.
- On syytä olettaa, että terveyspalvelujärjestelmän kannalta kustannustehokkaimpia ovat
- tehokas omahoitoon perustuva ehkäisy «Pattamatta M, Chapple I, Listl S. The value-for mo...»254
- parodontiitin riskiyksilöiden tunnistaminen ja hoidon kohdistaminen
- parodontiitin varhaisvaiheessa aloitettu hoito ja hoitotulosten ylläpito
- tupakoinnin aloittamisen ehkäisyyn tai lopettamiseen tähtäävät ohjelmat.
- Edellä mainitut toimenpiteet ehkäisevät parodontiitin aiheuttamia terveydellisiä ja psykososiaalisia haittoja «Needleman I, McGrath C, Floyd P, ym. Impact of ora...»255, «O'Dowd LK, Durham J, McCracken GI, ym. Patients' e...»256 ja mahdollistavat toimivan hampaiston säilyttämisen läpi elämän «Salvi GE, Mischler DC, Schmidlin K, ym. Risk facto...»257, «Braegger U. Cost-benefit, cost-effectiveness and c...»258, «Gjermo PE. Impact of periodontal preventive progra...»259, «Gaunt F, Devine M, Pennington M, ym. The cost-effe...»260.
- Hoidettujen omien hampaiden ennuste on parempi kuin hammasimplanttien «Tomasi C, Wennström JL, Berglundh T. Longevity of ...»261, «Holm-Pedersen P, Lang NP, Müller F. What are the l...»262, «Pjetursson BE, Heimisdottir K. Dental implants - a...»263, «Kupka JR, König J, Al-Nawas B, ym. How far can we ...»264.
- Omien hampaiden hoito on kustannustehokasta verrattuna implanttihoitoon.
- Implantin suuri hankintahinta vähentää sen kustannustehokkuutta.
- Oman hampaan ja implantin ylläpitohoito toteutuu potilaskohtaisesti samanlaisin perustein ja aikavälein riippumatta siitä, onko kyseessä implantti vai oma hammas. Siten ylläpitohoidosta potilaalle aiheutuvissa kustannuksissa ei ole eroa.
- Noin joka kolmannesta implantista seuraa komplikaatioita, jotka vaativat kirurgista hoitoa ja voivat pahimmillaan johtaa implantin poistoon «Derks J, Tomasi C. Peri-implant health and disease...»11, «Lee CT, Huang YW, Zhu L, ym. Prevalences of peri-i...»12, «Diaz P, Gonzalo E, Villagra LJG, ym. What is the p...»13, «Kordbacheh Changi K, Finkelstein J, Papapanou PN. ...»14.
Suomalaisen Lääkäriseuran Duodecimin ja Suomen Hammaslääkäriseura Apollonia ry:n asettama työryhmä
Parodontiitti-suosituksen historiatiedot «Parodontiitti, Käypä hoito -suosituksen historiatiedot»12
Puheenjohtaja:
Pekka Ylöstalo, parodontologian ja geriatrisen hammaslääketieteen professori; Oulun yliopisto
Jäsenet:
Mervi Gürsoy, parodontologian dosentti, HLT, EHL, yliopistonlehtori; Turun yliopisto
Mirkka Järvinen, FT, TtM, ammatillinen opettaja, suuhygienisti, toiminnanjohtaja; Suun terveydenhoidon ammattilaiset ry
Elisa Kopra, HLT, EHL, kliininen opettaja; Helsingin yliopisto, Suu- ja leukasairauksien osasto
Anu Marttala, EHL, ylihammaslääkäri; Länsi-Pohjan keskussairaala, Mehiläinen Länsi-Pohja Oy
Marja Pöllänen, parodontologian dosentti, HLT, EHL; Meritalon Hammaslääkärit Oy, Turku, Käypä hoito -toimittaja; Suomalainen Lääkäriseura Duodecim
Tuomas Saxlin, kliinisen parodontologian dosentti, HLT, EHL, kliininen opettaja; Itä-Suomen yliopisto
Asiantuntijat:
Anna Maria Heikkinen, suun terveydenhuollon professori, HLT, EHL, vastuualuejohtaja (erikoishoito, avopalvelut); Tampereen yliopisto, Pirkanmaan hyvinvointialue
Heidi Kuula, HLT, EHL, laatulääkäri; HUS Pää- ja kaulakeskus, Suusairauksien opetus- ja hoitoyksikkö
Hilkka Pernu, EHL; Oulun yliopisto
Sidonnaisuudet
Sidonnaisuusilmoitukset on tarkistettu 11.2.2025 julkaistun suosituksen laatimisen yhteydessä.
Mervi Gürsoy: Sivutoimet: ylihammaslääkäri; Suun terveydenhuolto, Varsinais-Suomen hyvinvointialue. Luottamustoimet terveydenhuollon alalla: puheenjohtaja, Parodontologian jaosto, koulutustoimikunnan jäsen, European Federation of Periodontology.
Mirkka Järvinen: Koulutus-, konsultointi- ja asiantuntijatoiminta: luentopalkkio: Denstal Oy, Nordic Healthcare Group, Apollonia, Qadental, YTHS, Turun Hammaslääkäriseura, Etelä-Pohjanmaan hyvinvointialue, Kymenlaakson hyvinvointialue, Lapin hyvinvointialue, Omnia, Pohjois-Pohjanmaan hyvinvointialue, Tehy ry, Länsi-Uudenmaan hyvinvointialue, Keusote. Ohjaushankkeet: Terveydenhuollon palveluvalikoimaneuvosto Palko, elintapajaosto 2020–2023, Suun tutkimus- ja hoitovälin määrittäminen Hyvä käytäntö -konsensussuositus 2023–2024, Osaamisen ennakointifoorumin Sosiaali-, terveys- ja hyvinvointiala -ennakointiryhmän asiantuntijaverkosto, 2022–2024, Alliance for Cavity-Free Future (ACFF), Suomen asiantuntijaryhmä.
Elisa Kopra: Sivutoimet: erikoishammaslääkäri; Helsingin kaupungin Suun erikoishoidon yksikkö, Ylioppilaiden terveydenhoitosäätiö, Oral Hammaslääkärit. Koulutus-, konsultointi- ja asiantuntijatoiminta: Suomen Hammaslääkäriseura Apollonia, QAdental, Oral Hammaslääkärit. Luottamustoimet terveydenhuollon alalla: Suomen Hammaslääkäriseura Apollonia Implantologian jaoston hallitus 2020–2024 ja koulutustoimikunta 2025–.
Anu Marttala: Ei aiheeseen liittyviä sidonnaisuuksia.
Marja Pöllänen: Luottamustoimet: STM, palveluvalikoimaneuvoston jäsen 30.6.2023 asti. Muut sidonnaisuudet: Meritalon Hammaslääkärit Oy, hallituksen puheenjohtaja.
Tuomas Saxlin: Sivutoimet: erikoishammaslääkäri; Pohjois-Savon hyvinvointialue ja PlusTerveys Oy Kuopion Hymyhammas. Koulutus-, konsultointi- ja asiantuntijatoiminta: luentopalkkio Golgate-Palmolive ja Hohde Group, kirjoituspalkkio Suomen Hammaslääkäriseura Apollonia ry. Luottamustoimet terveydenhuollon alalla: hallituksen jäsen, Suomen Hammaslääkäriliitto ry; vaaleja valmistelevan toimikunnan jäsen, varatoiminnantarkastaja 31.12.2023 asti, Suomen Hammaslääkäriseura Apollonia ry.
Pekka Ylöstalo: Sivutoimet: ylihammaslääkäri; Oulun yliopistollinen sairaala, konsultoiva erikoishammaslääkäri; Mehiläinen, Länsi-Pohjan keskussairaala, yksityinen ammatinharjoittaja.
Kirjallisuusviite
Parodontiitti. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Hammaslääkäriseura Apollonia ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2026 (viitattu pp.kk.vvvv). Saatavilla internetissä: www.kaypahoito.fi
Tarkemmat viittausohjeet: «http://www.kaypahoito.fi/web/kh/viittaaminen»9
Vastuun rajaus
Käypä hoito -suositukset ja Vältä viisaasti -suositukset ovat asiantuntijoiden laatimia yhteenvetoja yksittäisten sairauksien diagnostiikan ja hoidon vaikuttavuudesta. Suositukset toimivat lääkärin tai muun terveydenhuollon ammattilaisen päätöksenteon tukena hoitopäätöksiä tehtäessä. Ne eivät korvaa lääkärin tai muun terveydenhuollon ammattilaisen omaa arviota yksittäisen potilaan parhaasta mahdollisesta diagnostiikasta, hoidosta ja kuntoutuksesta hoitopäätöksiä tehtäessä.
Tiedonhakukäytäntö
Systemaattinen kirjallisuushaku on hoitosuosituksen perusta. Lue lisää artikkelista khk00007
Kirjallisuutta
- Hammasperäiset äkilliset infektiot ja mikrobilääkkeet. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Hammaslääkäriseura Apollonian asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2017 (viitattu 23.9.2024). Saatavilla internetissä: www.kaypahoito.fi
- Suominen L, Harjunmaa U. Suunterveyden tutkimus. Terve Suomi -ilmiöraportit. Sairaudet. https://www.thl.fi/tervesuomi_verkkoraportit/ilmioraportit_2023/suunterveys_syventava_tutkimus.html
- Terveys, toimintakyky ja hyvinvointi Suomessa 2011. Koskinen S, Lundqvist A, Ristiluoma N (toim.). https://www.julkari.fi/bitstream/handle/10024/90832/Rap068_2012_netti.pdf?sequence
- Nazir M, Al-Ansari A, Al-Khalifa K, ym. Global Prevalence of Periodontal Disease and Lack of Its Surveillance. ScientificWorldJournal 2020:2146160 «PMID: 32549797»PubMed
- Heikkinen AM, Pajukanta R, Pitkäniemi J, ym. The effect of smoking on periodontal health of 15- to 16-year-old adolescents. J Periodontol 2008;79(11):2042-7 «PMID: 18980511»PubMed
- Kassebaum NJ, Bernabé E, Dahiya M, ym. Global burden of severe periodontitis in 1990-2010: a systematic review and meta-regression. J Dent Res 2014;93(11):1045-53 «PMID: 25261053»PubMed
- Trindade D, Carvalho R, Machado V, ym. Prevalence of periodontitis in dentate people between 2011 and 2020: A systematic review and meta-analysis of epidemiological studies. J Clin Periodontol 2023;50(5):604-626 «PMID: 36631982»PubMed
- Saxén L. Juvenile periodontitis in Finland. Proc Finn Dent Soc 1987;83(3):143-9 «PMID: 3303023»PubMed
- Catunda RQ, Levin L, Kornerup I, ym. Prevalence of Periodontitis in Young Populations: A Systematic Review. Oral Health Prev Dent 2019;17(3):195-202 «PMID: 31209441»PubMed
- Jepsen S, Berglundh T, Genco R, ym. Primary prevention of peri-implantitis: managing peri-implant mucositis. J Clin Periodontol 2015;42 Suppl 16:S152-7 «PMID: 25626479»PubMed
- Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol 2015;42 Suppl 16:S158-71 «PMID: 25495683»PubMed
- Lee CT, Huang YW, Zhu L, ym. Prevalences of peri-implantitis and peri-implant mucositis: systematic review and meta-analysis. J Dent 2017;62:1-12 «PMID: 28478213»PubMed
- Diaz P, Gonzalo E, Villagra LJG, ym. What is the prevalence of peri-implantitis? A systematic review and meta-analysis. BMC Oral Health 2022;22(1):449 «PMID: 36261829»PubMed
- Kordbacheh Changi K, Finkelstein J, Papapanou PN. Peri-implantitis prevalence, incidence rate, and risk factors: A study of electronic health records at a U.S. dental school. Clin Oral Implants Res 2019;30(4):306-314 «PMID: 30768875»PubMed
- Reis INRD, do Amaral GCLS, Hassan MA, ym. The influence of smoking on the incidence of peri-implantitis: A systematic review and meta-analysis. Clin Oral Implants Res 2023;34(6):543-554 «PMID: 36939434»PubMed
- Axelsson P, Lindhe J. Effect of controlled oral hygiene procedures on caries and periodontal disease in adults. Results after 6 years. J Clin Periodontol 1981;8(3):239-48 «PMID: 6947990»PubMed
- Papapanou PN, Wennström JL. A 10-year retrospective study of periodontal disease progression. Clinical characteristics of subjects with pronounced and minimal disease development. J Clin Periodontol 1990;17(2):78-84 «PMID: 2303574»PubMed
- Lertpimonchai A, Rattanasiri S, Arj-Ong Vallibhakara S, ym. The association between oral hygiene and periodontitis: a systematic review and meta-analysis. Int Dent J 2017;67(6):332-343 «PMID: 28646499»PubMed
- Costa FO, Costa AM, Cortelli JR, ym. Effect of supragingival plaque control on recurrent periodontitis and clinical stability among individuals under periodontal maintenance therapy: 10-year follow-up. J Periodontol 2023;94(1):55-65 «PMID: 35904985»PubMed
- Bergstrom J. Smoking rate and periodontal disease prevalence: 40-year trends in Sweden 1970-2010. J Clin Periodontol 2014;41(10):952-7 «PMID: 25039432»PubMed
- Campos JR, Martins CC, Faria SFS, ym. Association between components of metabolic syndrome and periodontitis: a systematic review and meta-analysis. Clin Oral Investig 2022;26(9):5557-5574 «PMID: 35716205»PubMed
- Pirih FQ, Monajemzadeh S, Singh N, ym. Association between metabolic syndrome and periodontitis: The role of lipids, inflammatory cytokines, altered host response, and the microbiome. Periodontol 2000 2021;87(1):50-75 «PMID: 34463996»PubMed
- Jepsen S, Suvan J, Deschner J. The association of periodontal diseases with metabolic syndrome and obesity. Periodontol 2000 2020;83(1):125-153 «PMID: 32385882»PubMed
- Liu L, Xia LY, Gao YJ, ym. Association between Obesity and Periodontitis in US Adults: NHANES 2011-2014. Obes Facts 2024;17(1):47-58 «PMID: 37935140»PubMed
- Ylöstalo P, Suominen-Taipale L, Reunanen A, ym. Association between body weight and periodontal infection. J Clin Periodontol 2008;35(4):297-304 «PMID: 18294226»PubMed
- Kansanterveyslaitos. Suomalaisten aikuisten suunterveys. Terveys 2000 -tutkimus. Kansanterveyslaitoksen julkaisuja B16/2004:88-97, http://www.julkari.fi/bitstream/handle/10024/78322/2004b16.pdf
- Chambrone L, Chambrone D, Lima LA, ym. Predictors of tooth loss during long-term periodontal maintenance: a systematic review of observational studies. J Clin Periodontol 2010;37(7):675-84 «PMID: 20528960»PubMed
- Clark D, Kotronia E, Ramsay SE. Frailty, aging, and periodontal disease: Basic biologic considerations. Periodontol 2000 2021;87(1):143-156 «PMID: 34463998»PubMed
- Billings M, Holtfreter B, Papapanou PN, ym. Age-dependent distribution of periodontitis in two countries: Findings from NHANES 2009 to 2014 and SHIP-TREND 2008 to 2012. J Clin Periodontol 2018;45 Suppl 20:S130-S148 «PMID: 29926501»PubMed
- Hart TC, Atkinson JC. Mendelian forms of periodontitis. Periodontol 2000 2007;45:95-112 «PMID: 17850451»PubMed
- Deas DE, Mackey SA, McDonnell HT. Systemic disease and periodontitis: manifestations of neutrophil dysfunction. Periodontol 2000 2003;32:82-104 «PMID: 12756035»PubMed
- Uriarte SM, Hajishengallis G. Neutrophils in the periodontium: Interactions with pathogens and roles in tissue homeostasis and inflammation. Immunol Rev 2023;314(1):93-110 «PMID: 36271881»PubMed
- Nibali L, Bayliss-Chapman J, Almofareh SA, ym. What Is the Heritability of Periodontitis? A Systematic Review. J Dent Res 2019;98(6):632-641 «PMID: 31107142»PubMed
- Albandar JM, Susin C, Hughes FJ. Manifestations of systemic diseases and conditions that affect the periodontal attachment apparatus: Case definitions and diagnostic considerations. J Clin Periodontol 2018;45 Suppl 20:S171-S189 «PMID: 29926486»PubMed
- Hodge P, Michalowicz B. Genetic predisposition to periodontitis in children and young adults. Periodontol 2000 2001;26:113-34 «PMID: 11452901»PubMed
- Kinane DF, Hart TC. Genes and gene polymorphisms associated with periodontal disease. Crit Rev Oral Biol Med 2003;14(6):430-49 «PMID: 14656898»PubMed
- Loos BG, Papantonopoulos G, Jepsen S, ym. What is the Contribution of Genetics to Periodontal Risk? Dent Clin North Am 2015;59(4):761-80 «PMID: 26427567»PubMed
- Cepeda MS, Weinstein R, Blacketer C, ym. Association of flossing/inter-dental cleaning and periodontitis in adults. J Clin Periodontol 2017;44(9):866-871 «PMID: 28644512»PubMed
- Lipsky MS, Su S, Crespo CJ, ym. Men and Oral Health: A Review of Sex and Gender Differences. Am J Mens Health 2021;15(3):15579883211016361 «PMID: 33993787»PubMed
- Kocher T, Schwahn C, Gesch D, ym. Risk determinants of periodontal disease--an analysis of the Study of Health in Pomerania (SHIP 0). J Clin Periodontol 2005;32(1):59-67 «PMID: 15642060»PubMed
- Grbic JT, Lamster IB. Risk indicators for future clinical attachment loss in adult periodontitis. Tooth and site variables. J Periodontol 1992;63(4):262-9 «PMID: 1573540»PubMed
- Costa FO, Lages EJ, Cota LO, ym. Tooth loss in individuals under periodontal maintenance therapy: 5-year prospective study. J Periodontal Res 2014;49(1):121-8 «PMID: 23647520»PubMed
- Klinge B, Norlund A. A socio-economic perspective on periodontal diseases: a systematic review. J Clin Periodontol 2005;32 Suppl 6:314-25 «PMID: 16128846»PubMed
- Liang JH, Liu ML, Pu YQ, ym. Contribution of individual and cumulative social determinants of health underlying gender disparities in periodontitis in a representative US population: A cross-sectional NHANES study. J Clin Periodontol 2024;51(5):558-570 «PMID: 38200631»PubMed
- Knight ET, Liu J, Seymour GJ, ym. Risk factors that may modify the innate and adaptive immune responses in periodontal diseases. Periodontol 2000 2016;71(1):22-51 «PMID: 27045429»PubMed
- Könönen E, Paju S, Pussinen PJ, ym. Population-based study of salivary carriage of periodontal pathogens in adults. J Clin Microbiol 2007;45(8):2446-51 «PMID: 17567788»PubMed
- Ezzo PJ, Cutler CW. Microorganisms as risk indicators for periodontal disease. Periodontol 2000 2003;32:24-35 «PMID: 12756031»PubMed
- Haffajee AD, Socransky SS, Smith C, ym. Relation of baseline microbial parameters to future periodontal attachment loss. J Clin Periodontol 1991;18(10):744-50 «PMID: 1661304»PubMed
- Paju S, Pussinen PJ, Suominen-Taipale L, ym. Detection of multiple pathogenic species in saliva is associated with periodontal infection in adults. J Clin Microbiol 2009;47(1):235-8 «PMID: 19020069»PubMed
- Manoil D, Parga A, Bostanci N, ym. Microbial diagnostics in periodontal diseases. Periodontol 2000 2024;95(1):176-193 «PMID: 38797888»PubMed
- Belibasakis GN, Belstrøm D, Eick S, ym. Periodontal microbiology and microbial etiology of periodontal diseases: Historical concepts and contemporary perspectives. Periodontol 2000 2023 «PMID: 36661184»PubMed
- Antezack A, Etchecopar-Etchart D, La Scola B, ym. New putative periodontopathogens and periodontal health-associated species: A systematic review and meta-analysis. J Periodontal Res 2023;58(5):893-906 «PMID: 37572051»PubMed
- Iniesta M, Chamorro C, Ambrosio N, ym. Subgingival microbiome in periodontal health, gingivitis and different stages of periodontitis. J Clin Periodontol 2023;50(7):905-920 «PMID: 36792073»PubMed
- Ji S, Kook JK, Park SN, ym. Characteristics of the Salivary Microbiota in Periodontal Diseases and Potential Roles of Individual Bacterial Species To Predict the Severity of Periodontal Disease. Microbiol Spectr 2023;11(3):e0432722 «PMID: 37191548»PubMed
- Clerehugh V, Worthington HV, Lennon MA, ym. Site progression of loss of attachment over 5 years in 14- to 19-year-old adolescents. J Clin Periodontol 1995;22(1):15-21 «PMID: 7706535»PubMed
- Schätzle M, Löe H, Ramseier CA, ym. Clinical course of chronic periodontitis: effect of lifelong light smoking (20 years) on loss of attachment and teeth. J Investig Clin Dent 2010;1(1):8-15 «PMID: 25427181»PubMed
- Machtei EE, Hausmann E, Dunford R, ym. Longitudinal study of predictive factors for periodontal disease and tooth loss. J Clin Periodontol 1999;26(6):374-80 «PMID: 10382577»PubMed
- Lang NP, Schätzle MA, Löe H. Gingivitis as a risk factor in periodontal disease. J Clin Periodontol 2009;36 Suppl 10:3-8 «PMID: 19432625»PubMed
- Albandar JM. Some predictors of radiographic alveolar bone height reduction over 6 years. J Periodontal Res 1990;25(3):186-92 «PMID: 2141878»PubMed
- Matuliene G, Pjetursson BE, Salvi GE, ym. Influence of residual pockets on progression of periodontitis and tooth loss: results after 11 years of maintenance. J Clin Periodontol 2008;35(8):685-95 «PMID: 18549447»PubMed
- Schätzle M, Faddy MJ, Cullinan MP, ym. The clinical course of chronic periodontitis: V. Predictive factors in periodontal disease. J Clin Periodontol 2009;36(5):365-71 «PMID: 19419434»PubMed
- Lang NP, Kiel RA, Anderhalden K. Clinical and microbiological effects of subgingival restorations with overhanging or clinically perfect margins. J Clin Periodontol 1983;10(6):563-78 «PMID: 6581173»PubMed
- Schwalm CA, Smith DE, Erickson JD. A clinical study of patients 1 to 2 years after placement of removable partial dentures. J Prosthet Dent 1977;38(4):380-91 «PMID: 333107»PubMed
- Reitemeier B, Hänsel K, Walter MH, ym. Effect of posterior crown margin placement on gingival health. J Prosthet Dent 2002;87(2):167-72 «PMID: 11854673»PubMed
- Schätzle M, Land NP, Anerud A, ym. The influence of margins of restorations of the periodontal tissues over 26 years. J Clin Periodontol 2001;28(1):57-64 «PMID: 11142668»PubMed
- Ercoli C, Caton JG. Dental prostheses and tooth-related factors. J Clin Periodontol 2018;45 Suppl 20:S207-S218 «PMID: 29926482»PubMed
- Matthews DC, Tabesh M. Detection of localized tooth-related factors that predispose to periodontal infections. Periodontol 2000 2004;34:136-50 «PMID: 14717860»PubMed
- Burgett FG, Ramfjord SP, Nissle RR, ym. A randomized trial of occlusal adjustment in the treatment of periodontitis patients. J Clin Periodontol 1992;19(6):381-7 «PMID: 1634627»PubMed
- Harrel SK, Nunn ME. The association of occlusal contacts with the presence of increased periodontal probing depth. J Clin Periodontol 2009;36(12):1035-42 «PMID: 19930093»PubMed
- Bernhardt O, Gesch D, Look JO, ym. The influence of dynamic occlusal interferences on probing depth and attachment level: results of the Study of Health in Pomerania (SHIP). J Periodontol 2006;77(3):506-16 «PMID: 16512766»PubMed
- Siow DSF, Goh EXJ, Ong MMA, ym. Risk factors for tooth loss and progression of periodontitis in patients undergoing periodontal maintenance therapy. J Clin Periodontol 2023;50(1):61-70 «PMID: 36065561»PubMed
- Saleh MHA, Mallala D, Alrmali A, ym. Residual vertical defects: risk of disease progression, retreatment rates, and cost: a retrospective analysis. Clin Oral Investig 2024;28(8):446 «PMID: 39052104»PubMed
- Schwarz F, Derks J, Monje A, ym. Peri-implantitis. J Clin Periodontol 2018;45 Suppl 20:S246-S266 «PMID: 29926484»PubMed
- Heitz-Mayfield LJ. Peri-implant diseases: diagnosis and risk indicators. J Clin Periodontol 2008;35(8 Suppl):292-304 «PMID: 18724857»PubMed
- Renvert S, Quirynen M. Risk indicators for peri-implantitis. A narrative review. Clin Oral Implants Res 2015;26 Suppl 11:15-44 «PMID: 26385619»PubMed
- Fretwurst T, Nelson K. Influence of Medical and Geriatric Factors on Implant Success: An Overview of Systematic Reviews. Int J Prosthodont 2021;34:s21-s26 «PMID: 33571324»PubMed
- Karbach J, Callaway A, Kwon YD, ym. Comparison of five parameters as risk factors for peri-mucositis. Int J Oral Maxillofac Implants 2009;24(3):491-6 «PMID: 19587872»PubMed
- Dalago HR, Schuldt Filho G, Rodrigues MA, ym. Risk indicators for Peri-implantitis. A cross-sectional study with 916 implants. Clin Oral Implants Res 2017;28(2):144-150 «PMID: 26754342»PubMed
- Dreyer H, Grischke J, Tiede C, ym. Epidemiology and risk factors of peri-implantitis: A systematic review. J Periodontal Res 2018;53(5):657-681 «PMID: 29882313»PubMed
- Heitz-Mayfield LJA, Salvi GE. Peri-implant mucositis. J Clin Periodontol 2018;45 Suppl 20:S237-S245 «PMID: 29926488»PubMed
- Romandini M, Lima C, Pedrinaci I, ym. Prevalence and risk/protective indicators of peri-implant diseases: A university-representative cross-sectional study. Clin Oral Implants Res 2021;32(1):112-122 «PMID: 33210772»PubMed
- Heitz-Mayfield LJ, Huynh-Ba G. History of treated periodontitis and smoking as risks for implant therapy. Int J Oral Maxillofac Implants 2009;24 Suppl:39-68 «PMID: 19885434»PubMed
- Sgolastra F, Petrucci A, Severino M, ym. Smoking and the risk of peri-implantitis. A systematic review and meta-analysis. Clin Oral Implants Res 2015;26(4):e62-e67 «PMID: 24438442»PubMed
- Schwarz F, Alcoforado G, Guerrero A, ym. Peri-implantitis: Summary and consensus statements of group 3. The 6th EAO Consensus Conference 2021. Clin Oral Implants Res 2021;32 Suppl 21:245-253 «PMID: 34642987»PubMed
- Grischke J, Szafrański SP, Muthukumarasamy U, ym. Removable denture is a risk indicator for peri-implantitis and facilitates expansion of specific periodontopathogens: a cross-sectional study. BMC Oral Health 2021;21(1):173 «PMID: 33794847»PubMed
- Kesar N, Weigl P, Nentwig GH, ym. Prevalence and risk of peri-implant diseases based on the type of prosthetic restoration: A retrospective study after 17 to 23 years. J Prosthet Dent 2023;130(5):690-697 «PMID: 35016794»PubMed
- Latimer JM, Gharpure AS, Kahng HJ, ym. Interproximal open contacts between implant restorations and adjacent natural teeth as a risk-indicator for peri-implant disease-A cross-sectional study. Clin Oral Implants Res 2021;32(5):598-607 «PMID: 33629375»PubMed
- Herrera D, Berglundh T, Schwarz F, ym. Prevention and treatment of peri-implant diseases-The EFP S3 level clinical practice guideline. J Clin Periodontol 2023;50 Suppl 26:4-76 «PMID: 37271498»PubMed
- Renvert S, Polyzois I. Risk indicators for peri-implant mucositis: a systematic literature review. J Clin Periodontol 2015;42 Suppl 16:S172-86 «PMID: 25496066»PubMed
- Mahardawi B, Jiaranuchart S, Damrongsirirat N, ym. The lack of keratinized mucosa as a risk factor for peri-implantitis: a systematic review and meta-analysis. Sci Rep 2023;13(1):3778 «PMID: 36882495»PubMed
- Carra MC, Blanc-Sylvestre N, Courtet A, ym. Primordial and primary prevention of peri-implant diseases: A systematic review and meta-analysis. J Clin Periodontol 2023;50 Suppl 26:77-112 «PMID: 36807599»PubMed
- Ravidà A, Arena C, Tattan M, ym. The role of keratinized mucosa width as a risk factor for peri-implant disease: A systematic review, meta-analysis, and trial sequential analysis. Clin Implant Dent Relat Res 2022;24(3):287-300 «PMID: 35298862»PubMed
- Quirynen M, Dadamio J, Van den Velde S, ym. Characteristics of 2000 patients who visited a halitosis clinic. J Clin Periodontol 2009;36(11):970-5 «PMID: 19811581»PubMed
- Sanz M, Bäumer A, Buduneli N, ym. Effect of professional mechanical plaque removal on secondary prevention of periodontitis and the complications of gingival and periodontal preventive measures: consensus report of group 4 of the 11th European Workshop on Periodontology on effective prevention of periodontal and peri-implant diseases. J Clin Periodontol 2015;42 Suppl 16:S214-20 «PMID: 25626357»PubMed
- Holmstrup P, Glick M. Treatment of periodontal disease in the immunodeficient patient. Periodontol 2000 2002;28:190-205 «PMID: 12013342»PubMed
- Tsaousoglou P, Chatzopoulos GS, Tsalikis L, ym. Prevalence and risk indicators of peri-implantitis: a university based cross-sectional study. Quintessence Int 2023;54(7):558-568 «PMID: 37139954»PubMed
- Bondon-Guitton E, Bagheri H, Montastruc JL. Drug-induced gingival overgrowth: a study in the French Pharmacovigilance Database. J Clin Periodontol 2012;39(6):513-8 «PMID: 22519416»PubMed
- Glick A, Sista V, Johnson C. Oral Manifestations of Commonly Prescribed Drugs. Am Fam Physician 2020;102(10):613-621 «PMID: 33179891»PubMed
- Sälzer S, Slot DE, Van der Weijden FA, ym. Efficacy of inter-dental mechanical plaque control in managing gingivitis--a meta-review. J Clin Periodontol 2015;42 Suppl 16:S92-105 «PMID: 25581718»PubMed
- Martins CC, Lockhart PB, Firmino RT, ym. Bacteremia following different oral procedures: Systematic review and meta-analysis. Oral Dis 2024;30(3):846-854 «PMID: 36750413»PubMed
- Viisaudenhammas. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Hammaslääkäriseura Apollonia ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2020 (viitattu 23.9.2024). Saatavilla internetissä: www.kaypahoito.fi
- Blakey GH, Marciani RD, Haug RH, ym. Periodontal pathology associated with asymptomatic third molars. J Oral Maxillofac Surg 2002;60(11):1227-33 «PMID: 12420253»PubMed
- Offenbacher S, Beck JD, Moss KL, ym. What are the local and systemic implications of third molar retention? J Oral Maxillofac Surg 2012;70(9 Suppl 1):S58-65 «PMID: 22916700»PubMed
- Valtioneuvoston asetus neuvolatoiminnasta, koulu- ja opiskeluterveydenhuollosta sekä lasten ja nuorten ehkäisevästä suun terveydenhuollosta. 338/2011. Viitattu 23.9.2024. http://www.finlex.fi/fi/laki/alkup/2011/20110338
- Tupakka- ja nikotiiniriippuvuuden ehkäisy ja hoito. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Yleislääketieteen yhdistyksen asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu 23.9.2024). Saatavilla internetissä: www.kaypahoito.fi
- Suun tutkimus- ja hoitovälin määrittäminen Hyvä käytäntö -konsensussuositus. Hietala-Lenkkeri A, Raudasoja A, Pöllänen M, Suomalaisen Lääkäriseuran Duodecimin ja Suomen Hammaslääkäriseuran Apollonian nimittämän konsensussuosituspaneelin puolesta. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu 23.9.2024). Saatavilla internetissä: www.kaypahoito.fi
- Nieminen M, Varrela T, Könönen E ym. Furkaatioleesioiden etiologia, diagnostiikka ja hoito. Suom Hammaslääkäril 2015;(8):20-8
- Lindhe J, Meyle J, Group D of European Workshop on Periodontology. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J Clin Periodontol 2008;35(8 Suppl):282-5 «PMID: 18724855»PubMed
- Caton JG, Armitage G, Berglundh T, ym. A new classification scheme for periodontal and peri-implant diseases and conditions - Introduction and key changes from the 1999 classification. J Periodontol 2018;89 Suppl 1:S1-S8 «PMID: 29926946»PubMed
- Jepsen S, Caton JG, Albandar JM, ym. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol 2018;89 Suppl 1:S237-S248 «PMID: 29926943»PubMed
- Avila-Ortiz G, Gonzalez-Martin O, Couso-Queiruga E, ym. The peri-implant phenotype. J Periodontol 2020;91(3):283-288 «PMID: 32027021»PubMed
- Larsen C, Barendregt DS, Slot DE, ym. Probing pressure, a highly undervalued unit of measure in periodontal probing: a systematic review on its effect on probing pocket depth. J Clin Periodontol 2009;36(4):315-22 «PMID: 19426178»PubMed
- Bulthuis HM, Barendregt DS, Timmerman MF, ym. Probe penetration in relation to the connective tissue attachment level: influence of tine shape and probing force. J Clin Periodontol 1998;25(5):417-23 «PMID: 9650880»PubMed
- Wang SF, Leknes KN, Zimmerman GJ, ym. Reproducibility of periodontal probing using a conventional manual and an automated force-controlled electronic probe. J Periodontol 1995;66(1):38-46 «PMID: 7891248»PubMed
- Grossi SG, Dunford RG, Ho A, ym. Sources of error for periodontal probing measurements. J Periodontal Res 1996;31(5):330-6 «PMID: 8858537»PubMed
- Scott DA, Singer DL. Suppression of overt gingival inflammation in tobacco smokers - clinical and mechanistic considerations. Int J Dent Hyg 2004;2(3):104-10 «PMID: 16451473»PubMed
- Lang NP, Adler R, Joss A, ym. Absence of bleeding on probing. An indicator of periodontal stability. J Clin Periodontol 1990;17(10):714-21 «PMID: 2262585»PubMed
- Pepelassi EA, Tsiklakis K, Diamanti-Kipioti A. Radiographic detection and assessment of the periodontal endosseous defects. J Clin Periodontol 2000;27(4):224-30 «PMID: 10783834»PubMed
- Preshaw PM. Detection and diagnosis of periodontal conditions amenable to prevention. BMC Oral Health 2015;15 Suppl 1(Suppl 1):S5 «PMID: 26390822»PubMed
- Graetz C, Plaumann A, Wiebe JF, ym. Periodontal probing versus radiographs for the diagnosis of furcation involvement. J Periodontol 2014;85(10):1371-9 «PMID: 24605872»PubMed
- Whaites E, Drage N. Essentials at Dental Radiography and Radiology, 6th ed. 2021: Bitewing Radiography. Essentials of Dental Radiography and Radiology, 10, 125-133. Diagrams showing the ideal image receptor positions for different types of bitewings.
- Wei S, Lin T, Sáenz-Ravello G, ym. Diagnostic accuracy of salivary active matrix metalloproteinase (aMMP)-8 point-of-care test for detecting periodontitis in adults: A systematic review and meta-analysis. J Clin Periodontol 2024;51(8):1093-1108 «PMID: 38763168»PubMed
- Deng K, Pelekos G, Jin L, ym. Diagnostic accuracy of a point-of-care aMMP-8 test in the discrimination of periodontal health and disease. J Clin Periodontol 2021;48(8):1051-1065 «PMID: 33998040»PubMed
- Buduneli N, Bıyıkoğlu B, Kinane DF. Utility of gingival crevicular fluid components for periodontal diagnosis. Periodontol 2000 2024;95(1):156-175 «PMID: 39004819»PubMed
- Ebersole JL, Hasturk H, Huber M, ym. Realizing the clinical utility of saliva for monitoring oral diseases. Periodontol 2000 2024;95(1):203-219 «PMID: 39010260»PubMed
- Holmstrup P, Plemons J, Meyle J. Non-plaque-induced gingival diseases. J Clin Periodontol 2018;45 Suppl 20:S28-S43 «PMID: 29926497»PubMed
- Chapple ILC, Mealey BL, Van Dyke TE, ym. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol 2018;45 Suppl 20:S68-S77 «PMID: 29926499»PubMed
- Trombelli L, Farina R, Silva CO, ym. Plaque-induced gingivitis: Case definition and diagnostic considerations. J Clin Periodontol 2018;45 Suppl 20:S44-S67 «PMID: 29926492»PubMed
- Papapanou PN, Sanz M, Buduneli N, ym. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol 2018;45 Suppl 20:S162-S170 «PMID: 29926490»PubMed
- Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Clin Periodontol 2018;45 Suppl 20:S149-S161 «PMID: 29926495»PubMed
- Berglundh T, Armitage G, Araujo MG, ym. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol 2018;45 Suppl 20:S286-S291 «PMID: 29926491»PubMed
- Renvert S, Persson GR, Pirih FQ, ym. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J Clin Periodontol 2018;45 Suppl 20:S278-S285 «PMID: 29926496»PubMed
- Mombelli A, Gusberti FA, van Oosten MA, ym. Gingival health and gingivitis development during puberty. A 4-year longitudinal study. J Clin Periodontol 1989;16(7):451-6 «PMID: 2768539»PubMed
- Nakagawa S, Fujii H, Machida Y, ym. A longitudinal study from prepuberty to puberty of gingivitis. Correlation between the occurrence of Prevotella intermedia and sex hormones. J Clin Periodontol 1994;21(10):658-65 «PMID: 7852609»PubMed
- Figuero E, Carrillo-de-Albornoz A, Martín C, ym. Effect of pregnancy on gingival inflammation in systemically healthy women: a systematic review. J Clin Periodontol 2013;40(5):457-73 «PMID: 23557432»PubMed
- Gürsoy M, Pajukanta R, Sorsa T, ym. Clinical changes in periodontium during pregnancy and post-partum. J Clin Periodontol 2008;35(7):576-83 «PMID: 18430046»PubMed
- Trackman PC, Kantarci A. Connective tissue metabolism and gingival overgrowth. Crit Rev Oral Biol Med 2004;15(3):165-75 «PMID: 15187034»PubMed
- Seymour RA. Effects of medications on the periodontal tissues in health and disease. Periodontol 2000 2006;40:120-9 «PMID: 16398689»PubMed
- Tonetti MS, Sanz M. Implementation of the new classification of periodontal diseases: Decision-making algorithms for clinical practice and education. J Clin Periodontol 2019;46(4):398-405 «PMID: 30883878»PubMed
- Fine DH, Patil AG, Loos BG. Classification and diagnosis of aggressive periodontitis. J Clin Periodontol 2018;45 Suppl 20:S95-S111 «PMID: 29926487»PubMed
- Kornman KS, Papapanou PN. Clinical application of the new classification of periodontal diseases: Ground rules, clarifications and "gray zones". J Periodontol 2020;91(3):352-360 «PMID: 31891194»PubMed
- Dietrich T, Ower P, Tank M, ym. Periodontal diagnosis in the context of the 2017 classification system of periodontal diseases and conditions - implementation in clinical practice. Br Dent J 2019;226(1):16-22 «PMID: 30631188»PubMed
- Sanz M, Herrera D, Kebschull M, ym. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J Clin Periodontol 2020;47 Suppl 22:4-60 «PMID: 32383274»PubMed
- Pitchika V, Pink C, Völzke H, ym. Long-term impact of powered toothbrush on oral health: 11-year cohort study. J Clin Periodontol 2019;46(7):713-722 «PMID: 31115952»PubMed
- Davidovich E, Shafir S, Shay B, ym. Plaque Removal by a Powered Toothbrush Versus a Manual Toothbrush in Children: A Systematic Review and Meta-Analysis. Pediatr Dent 2020;42(4):280-287 «PMID: 32847667»PubMed
- Löe H, Morrison E. Periodontal health and disease in young people: screening for priority care. Int Dent J 1986;36(3):162-7 «PMID: 3533788»PubMed
- Tonetti MS, Chapple IL, Jepsen S, ym. Primary and secondary prevention of periodontal and peri-implant diseases: Introduction to, and objectives of the 11th European Workshop on Periodontology consensus conference. J Clin Periodontol 2015;42 Suppl 16:S1-4 «PMID: 25683242»PubMed
- Sambunjak D, Nickerson JW, Poklepovic T, ym. Flossing for the management of periodontal diseases and dental caries in adults. Cochrane Database Syst Rev 2011;(12):CD008829 «PMID: 22161438»PubMed
- van der Weijden F, Slot DE, van der Sluijs E, ym. The efficacy of a rubber bristles interdental cleaner on parameters of oral soft tissue health-a systematic review. Int J Dent Hyg 2022;20(1):26-39 «PMID: 33630360»PubMed
- Sälzer S, Graetz C, Dörfer CE, ym. Contemporary practices for mechanical oral hygiene to prevent periodontal disease. Periodontol 2000 2020;84(1):35-44 «PMID: 32844413»PubMed
- Yost KG, Mallatt ME, Liebman J. Interproximal gingivitis and plaque reduction by four interdental products. J Clin Dent 2006;17(3):79-83 «PMID: 17022370»PubMed
- Abouassi T, Woelber JP, Holst K, ym. Clinical efficacy and patients' acceptance of a rubber interdental bristle. A randomized controlled trial. Clin Oral Investig 2014;18(7):1873-80 «PMID: 24407549»PubMed
- Slot DE, Valkenburg C, Van der Weijden GAF. Mechanical plaque removal of periodontal maintenance patients: A systematic review and network meta-analysis. J Clin Periodontol 2020;47 Suppl 22:107-124 «PMID: 32716118»PubMed
- Taschieri S, Tumedei M, Francetti L, ym. Efficacy of 67% sodium bicarbonate toothpaste for plaque and gingivitis control: a systematic review and meta-analysis. J Evid Based Dent Pract 2022;22(2):101709 «PMID: 35718441»PubMed
- Valkenburg C, Van der Weijden FA, Slot DE. Plaque control and reduction of gingivitis: The evidence for dentifrices. Periodontol 2000 2019;79(1):221-232 «PMID: 30892760»PubMed
- Lindson N, Thompson TP, Ferrey A, ym. Motivational interviewing for smoking cessation. Cochrane Database Syst Rev 2019;7(7):CD006936 «PMID: 31425622»PubMed
- Ramseier CA, Suvan JE. Behaviour change counselling for tobacco use cessation and promotion of healthy lifestyles: a systematic review. J Clin Periodontol 2015;42 Suppl 16:S47-58 «PMID: 25496370»PubMed
- Werner H, Hakeberg M, Dahlström L, ym. Psychological Interventions for Poor Oral Health: A Systematic Review. J Dent Res 2016;95(5):506-14 «PMID: 26826109»PubMed
- Hugoson A, Lundgren D, Asklöw B, ym. Effect of three different dental health preventive programmes on young adult individuals: a randomized, blinded, parallel group, controlled evaluation of oral hygiene behaviour on plaque and gingivitis. J Clin Periodontol 2007;34(5):407-15 «PMID: 17448044»PubMed
- Hujoel PP, Cunha-Cruz J, Loesche WJ, ym. Personal oral hygiene and chronic periodontitis: a systematic review. Periodontol 2000 2005;37:29-34 «PMID: 15655023»PubMed
- Needleman I, Nibali L, Di Iorio A. Professional mechanical plaque removal for prevention of periodontal diseases in adults--systematic review update. J Clin Periodontol 2015;42 Suppl 16:S12-35 «PMID: 25495962»PubMed
- Gómez-Moreno G, Aguilar-Salvatierra A, Rubio Roldán J, ym. Peri-implant evaluation in type 2 diabetes mellitus patients: a 3-year study. Clin Oral Implants Res 2015;26(9):1031-5 «PMID: 24684438»PubMed
- Monje A, Aranda L, Diaz KT, ym. Impact of Maintenance Therapy for the Prevention of Peri-implant Diseases: A Systematic Review and Meta-analysis. J Dent Res 2016;95(4):372-9 «PMID: 26701350»PubMed
- Verket A, Koldsland OC, Bunaes D, ym. Non-surgical therapy of peri-implant mucositis-Mechanical/physical approaches: A systematic review. J Clin Periodontol 2023;50 Suppl 26:135-145 «PMID: 36802083»PubMed
- Romandini M, Lima C, Pedrinaci I, ym. Prevalence and risk/protective indicators of peri-implant diseases: A university-representative cross-sectional study. Clin Oral Implants Res 2021;32(1):112-122 «PMID: 33210772»PubMed
- al-Tannir MA, Goodman HS. A review of chlorhexidine and its use in special populations. Spec Care Dentist 1994;14(3):116-22 «PMID: 7871472»PubMed
- Moazzez R, Thompson H, Palmer RM, ym. Effect of rinsing with ethanol-containing mouthrinses on the production of salivary acetaldehyde. Eur J Oral Sci 2011;119(6):441-6 «PMID: 22112029»PubMed
- Chevalier M, Sakarovitch C, Precheur I, ym. Antiseptic mouthwashes could worsen xerostomia in patients taking polypharmacy. Acta Odontol Scand 2015;73(4):267-73 «PMID: 25601200»PubMed
- Bondonno CP, Liu AH, Croft KD, ym. Antibacterial mouthwash blunts oral nitrate reduction and increases blood pressure in treated hypertensive men and women. Am J Hypertens 2015;28(5):572-5 «PMID: 25359409»PubMed
- Aceves Argemí R, González Navarro B, Ochoa García-Seisdedos P, ym. Mouthwash With Alcohol and Oral Carcinogenesis: Systematic Review and Meta-analysis. J Evid Based Dent Pract 2020;20(2):101407 «PMID: 32473798»PubMed
- Ustrell-Borràs M, Traboulsi-Garet B, Gay-Escoda C. Alcohol-based mouthwash as a risk factor of oral cancer: A systematic review. Med Oral Patol Oral Cir Bucal 2020;25(1):e1-e12 «PMID: 31655832»PubMed
- Carneiro CMM, Pinho PS, Teixeira JRB, ym. Unpaid domestic work: persistence of gender-based labor division and mental disorders. Rev Saude Publica 2023;57:31 «PMID: 37283399»PubMed
- Ramseier CA, Woelber JP, Kitzmann J, ym. Impact of risk factor control interventions for smoking cessation and promotion of healthy lifestyles in patients with periodontitis: A systematic review. J Clin Periodontol 2020;47 Suppl 22:90-106 «PMID: 31912512»PubMed
- Carra MC, Detzen L, Kitzmann J, ym. Promoting behavioural changes to improve oral hygiene in patients with periodontal diseases: A systematic review. J Clin Periodontol 2020;47 Suppl 22:72-89 «PMID: 31912530»PubMed
- Worthington HV, MacDonald L, Poklepovic Pericic T, ym. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database Syst Rev 2019;4(4):CD012018 «PMID: 30968949»PubMed
- Chapple IL, Van der Weijden F, Doerfer C, ym. Primary prevention of periodontitis: managing gingivitis. J Clin Periodontol 2015;42 Suppl 16:S71-6 «PMID: 25639826»PubMed
- Van der Weijden FA, Slot DE. Efficacy of homecare regimens for mechanical plaque removal in managing gingivitis a meta review. J Clin Periodontol 2015;42 Suppl 16:S77-91 «PMID: 25597787»PubMed
- Ravidà A, Troiano G, Qazi M, ym. Dose-dependent effect of smoking and smoking cessation on periodontitis-related tooth loss during 10 - 47 years periodontal maintenance-A retrospective study in compliant cohort. J Clin Periodontol 2020;47(9):1132-1143 «PMID: 32593185»PubMed
- Tyypin 2 diabetes. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin, Suomen Sisätautilääkärien yhdistyksen ja Diabetesliiton Lääkärineuvoston asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2024 (viitattu 23.9.2024). Saatavilla internetissä: www.kaypahoito.fi
- Suvan J, Leira Y, Moreno Sancho FM, ym. Subgingival instrumentation for treatment of periodontitis. A systematic review. J Clin Periodontol 2020;47 Suppl 22:155-175 «PMID: 31889320»PubMed
- Newman MG, Elangovan S, Dragan IF ym. Nonsurgical periodontal therapy. Teoksessa: Newman and Carranza’s Essentials of Clinical Periodontology, Vol 1, E-kirja, Elsevier Inc 2022 (viitattu 16.12.2024).
- Jervøe-Storm PM, Eberhard J, Needleman I, ym. Full-mouth treatment modalities (within 24 hours) for periodontitis in adults. Cochrane Database Syst Rev 2022;6(6):CD004622 «PMID: 35763286»PubMed
- Graziani F, Cei S, Orlandi M, ym. Acute-phase response following full-mouth versus quadrant non-surgical periodontal treatment: A randomized clinical trial. J Clin Periodontol 2015;42(9):843-852 «PMID: 26309133»PubMed
- da Costa LFNP, Amaral CDSF, Barbirato DDS, ym. Chlorhexidine mouthwash as an adjunct to mechanical therapy in chronic periodontitis: A meta-analysis. J Am Dent Assoc 2017;148(5):308-318 «PMID: 28284417»PubMed
- James P, Worthington HV, Parnell C, ym. Chlorhexidine mouthrinse as an adjunctive treatment for gingival health. Cochrane Database Syst Rev 2017;3(3):CD008676 «PMID: 28362061»PubMed
- Teughels W, Feres M, Oud V, ym. Adjunctive effect of systemic antimicrobials in periodontitis therapy: A systematic review and meta-analysis. J Clin Periodontol 2020;47 Suppl 22:257-281 «PMID: 31994207»PubMed
- Mombelli A, Almaghlouth A, Cionca N, ym. Differential benefits of amoxicillin-metronidazole in different phases of periodontal therapy in a randomized controlled crossover clinical trial. J Periodontol 2015;86(3):367-75 «PMID: 25415250»PubMed
- Donos N, Calciolari E, Brusselaers N, ym. The adjunctive use of host modulators in non-surgical periodontal therapy. A systematic review of randomized, placebo-controlled clinical studies. J Clin Periodontol 2020;47 Suppl 22:199-238 «PMID: 31834951»PubMed
- Helal O, Göstemeyer G, Krois J, ym. Predictors for tooth loss in periodontitis patients: Systematic review and meta-analysis. J Clin Periodontol 2019;46(7):699-712 «PMID: 31025366»PubMed
- Chen X, Xu C, Wu Y, ym. The survival of periodontally treated molars in long-term maintenance: A systematic review and meta-analysis. J Clin Periodontol 2024;51(5):631-651 «PMID: 38317331»PubMed
- Dawood A, Patel S. The Dental Practicality Index - assessing the restorability of teeth. Br Dent J 2017;222(10):755-758 «PMID: 28546619»PubMed
- Dommisch H, Walter C, Dannewitz B, ym. Resective surgery for the treatment of furcation involvement: A systematic review. J Clin Periodontol 2020;47 Suppl 22:375-391 «PMID: 31912534»PubMed
- Jepsen S, Gennai S, Hirschfeld J, ym. Regenerative surgical treatment of furcation defects: A systematic review and Bayesian network meta-analysis of randomized clinical trials. J Clin Periodontol 2020;47 Suppl 22:352-374 «PMID: 31860125»PubMed
- Nationella riktlinjer för tandvård. Stöd för styrning och ledning 2022. https://www.socialstyrelsen.se/kunskapsstod-och-regler/regler-och-riktlinjer/nationella-riktlinjer/riktlinjer-och-utvarderingar/tandvard/
- Patel RA, Wilson RF, Palmer RM. The effect of smoking on periodontal bone regeneration: a systematic review and meta-analysis. J Periodontol 2012;83(2):143-55 «PMID: 21627463»PubMed
- von Troil B, Needleman I, Sanz M. A systematic review of the prevalence of root sensitivity following periodontal therapy. J Clin Periodontol 2002;29 Suppl 3:173-7; discussion 195-6 «PMID: 12787217»PubMed
- Liu XX, Tenenbaum HC, Wilder RS, ym. Pathogenesis, diagnosis and management of dentin hypersensitivity: an evidence-based overview for dental practitioners. BMC Oral Health 2020;20(1):220 «PMID: 32762733»PubMed
- Dommisch H, Walter C, Difloe-Geisert JC, ym. Efficacy of tooth splinting and occlusal adjustment in patients with periodontitis exhibiting masticatory dysfunction: A systematic review. J Clin Periodontol 2022;49 Suppl 24:149-166 «PMID: 34854115»PubMed
- Carra MC, Rangé H, Swerts PJ, ym. Effectiveness of implant-supported fixed partial denture in patients with history of periodontitis: A systematic review and meta-analysis. J Clin Periodontol 2022;49 Suppl 24:208-223 «PMID: 34775625»PubMed
- Gotfredsen K, Rimborg S, Stavropoulos A. Efficacy and risks of removable partial prosthesis in periodontitis patients: A systematic review. J Clin Periodontol 2022;49 Suppl 24:167-181 «PMID: 34761421»PubMed
- Montero E, Molina A, Palombo D, ym. Efficacy and risks of tooth-supported prostheses in the treatment of partially edentulous patients with stage IV periodontitis. A systematic review and meta-analysis. J Clin Periodontol 2022;49 Suppl 24:182-207 «PMID: 34786742»PubMed
- Herrera D, Sanz M, Kebschull M, ym. Treatment of stage IV periodontitis: The EFP S3 level clinical practice guideline. J Clin Periodontol 2022;49 Suppl 24:4-71 «PMID: 35688447»PubMed
- Martin C, Celis B, Ambrosio N, ym. Effect of orthodontic therapy in periodontitis and non-periodontitis patients: a systematic review with meta-analysis. J Clin Periodontol 2022;49 Suppl 24:72-101 «PMID: 33998045»PubMed
- Paternò Holtzman L, Valente NA, Vittorini Orgeas G, ym. Change in clinical parameters after subgingival instrumentation for the treatment of periodontitis and timing of periodontal re-evaluation: A systematic review and meta-analysis. J Clin Periodontol 2025;52(1):137-158 «PMID: 38706227»PubMed
- Saydzai S, Buontempo Z, Patel P, ym. Comparison of the efficacy of periodontal prognostic systems in predicting tooth loss. J Clin Periodontol 2022;49(8):740-748 «PMID: 35702014»PubMed
- Sonnenschein SK, Betzler C, Rütters MA, ym. Long-term stability of splinted anterior mandibular teeth during supportive periodontal therapy. Acta Odontol Scand 2017;75(7):475-482 «PMID: 28643542»PubMed
- Tomasi C, Leyland AH, Wennström JL. Factors influencing the outcome of non-surgical periodontal treatment: a multilevel approach. J Clin Periodontol 2007;34(8):682-90 «PMID: 17635246»PubMed
- Rattu V, Raindi D, Antonoglou G, ym. Prevalence of stable and successfully treated periodontitis subjects and incidence of subsequent tooth loss within supportive periodontal care: A systematic review with meta-analyses. J Clin Periodontol 2023;50(10):1371-1389 «PMID: 37402624»PubMed
- Feres M, Retamal-Valdes B, Faveri M, ym. Proposal of a Clinical Endpoint for Periodontal Trials: The Treat-to-Target Approach. J Int Acad Periodontol 2020;22(2):41-53 «PMID: 32224549»PubMed
- Sanz-Sánchez I, Montero E, Citterio F, ym. Efficacy of access flap procedures compared to subgingival debridement in the treatment of periodontitis. A systematic review and meta-analysis. J Clin Periodontol 2020;47 Suppl 22:282-302 «PMID: 31970821»PubMed
- Ramseier CA, Nydegger M, Walter C, ym. Time between recall visits and residual probing depths predict long-term stability in patients enrolled in supportive periodontal therapy. J Clin Periodontol 2019;46(2):218-230 «PMID: 30499586»PubMed
- Cosgarea R, Roccuzzo A, Jepsen K, ym. Efficacy of mechanical/physical approaches for implant surface decontamination in non-surgical submarginal instrumentation of peri-implantitis. A systematic review. J Clin Periodontol 2023;50 Suppl 26:188-211 «PMID: 36550060»PubMed
- de Waal YCM, Winning L, Stavropoulos A, ym. Efficacy of chemical approaches for implant surface decontamination in conjunction with sub-marginal instrumentation, in the non-surgical treatment of peri-implantitis: A systematic review. J Clin Periodontol 2023;50 Suppl 26:212-223 «PMID: 36375830»PubMed
- Liñares A, Sanz-Sánchez I, Dopico J, ym. Efficacy of adjunctive measures in the non-surgical treatment of peri-implantitis: A systematic review. J Clin Periodontol 2023;50 Suppl 26:224-243 «PMID: 37143407»PubMed
- Trombelli L, Franceschetti G, Farina R. Effect of professional mechanical plaque removal performed on a long-term, routine basis in the secondary prevention of periodontitis: a systematic review. J Clin Periodontol 2015;42 Suppl 16:S221-36 «PMID: 25495875»PubMed
- Herrera D, Retamal-Valdes B, Alonso B, ym. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J Clin Periodontol 2018;45 Suppl 20:S78-S94 «PMID: 29926493»PubMed
- Herrera D, Roldán S, González I, ym. The periodontal abscess (I). Clinical and microbiological findings. J Clin Periodontol 2000;27(6):387-94 «PMID: 10883867»PubMed
- Herrera D, Feres M. Treatment of acute periodontal and endo-periodontal lesions. Teoksessa: Lang NP, Berglundh T, Giannobible WV ym. (toim): Lindhe’s Clinical Periodontology and Implantology, Vol 2, E-kirja. Wiley-Blackwell 2022
- Hampaan juurihoito. Käypä hoito -suositus. Suomalaisen Lääkäriseuran Duodecimin ja Suomen Hammaslääkäriseura Apollonia ry:n asettama työryhmä. Helsinki: Suomalainen Lääkäriseura Duodecim, 2022 (viitattu 23.9.2024). Saatavilla internetissä: www.kaypahoito.fi
- Nibali L, Pometti D, Chen TT, ym. Minimally invasive non-surgical approach for the treatment of periodontal intrabony defects: a retrospective analysis. J Clin Periodontol 2015;42(9):853-859 «PMID: 26257238»PubMed
- Kučič AC, Gašperšič R. Minimally invasive non-surgical therapy (MINST) in stage III periodontitis patients: 6-month results of a split-mouth, randomised controlled clinical trial. Clin Oral Investig 2023;27(5):2075-2087 «PMID: 37014505»PubMed
- Ng E, Tay JRH, Ong MMA. Minimally Invasive Periodontology: A Treatment Philosophy and Suggested Approach. Int J Dent 2021:2810264 «PMID: 34257659»PubMed
- Ribeiro FV, Mehta JJ, Monteiro MF, ym. Minimal invasiveness in nonsurgical periodontal therapy. Periodontol 2000 2023;91(1):7-19 «PMID: 36661203»PubMed
- Nibali L, Yeh YC, Pometti D, ym. Long-term stability of intrabony defects treated with minimally invasive non-surgical therapy. J Clin Periodontol 2018;45(12):1458-1464 «PMID: 30307641»PubMed
- Gupta S, Tewari S, Tewari S, ym. Effect of Time Lapse between Endodontic and Periodontal Therapies on the Healing of Concurrent Endodontic-Periodontal Lesions without Communication: A Prospective Randomized Clinical Trial. J Endod 2015;41(6):785-90 «PMID: 25817213»PubMed
- Cortellini P, Stalpers G, Mollo A, ym. Periodontal regeneration versus extraction and dental implant or prosthetic replacement of teeth severely compromised by attachment loss to the apex: A randomized controlled clinical trial reporting 10-year outcomes, survival analysis and mean cumulative cost of recurrence. J Clin Periodontol 2020;47(6):768-776 «PMID: 32249446»PubMed
- AlJasser R, Bukhary S, AlSarhan M, ym. Regenerative Therapy Modality for Treatment of True Combined Endodontic-Periodontal Lesions: A Randomized Controlled Clinical Trial. Int J Environ Res Public Health 2021;18(12):6220 «PMID: 34201328»PubMed
- Fan X, Xu X, Yu S, ym. Prognostic Factors of Grade 2-3 Endo-Periodontal Lesions Treated Nonsurgically in Patients with Periodontitis: A Retrospective Case-Control Study. Biomed Res Int 2020:1592910 «PMID: 32090068»PubMed
- Pastagia J, Nicoara P, Robertson PB. The effect of patient-centered plaque control and periodontal maintenance therapy on adverse outcomes of periodontitis. J Evid Based Dent Pract 2006;6(1):25-32 «PMID: 17138393»PubMed
- Paśnik-Chwalik B, Konopka T. Impact of periodontitis on the Oral Health Impact Profile: A systematic review and meta-analysis. Dent Med Probl 2020;57(4):423-431 «PMID: 33263952»PubMed
- Raval P, Moreno F, Needleman I. Patient involvement to explore research prioritisation and self-care management in people with periodontitis and diabetes. Br Dent J 2021 Jul 8 «PMID: 34239054»PubMed
- Mendez M, Melchiors Angst PD, Stadler AF, ym. Impacts of supragingival and subgingival periodontal treatments on oral health-related quality of life. Int J Dent Hyg 2017;15(2):135-141 «PMID: 26799625»PubMed
- Rawlinson A, Vettore MV, Baker SR, ym. Periodontal treatment, psychological factors and oral health-related quality of life. J Clin Periodontol 2021;48(2):226-236 «PMID: 33263182»PubMed
- Paraskevas S, Huizinga JD, Loos BG. A systematic review and meta-analyses on C-reactive protein in relation to periodontitis. J Clin Periodontol 2008;35(4):277-90 «PMID: 18294231»PubMed
- Lalla E, Papapanou PN. Diabetes mellitus and periodontitis: a tale of two common interrelated diseases. Nat Rev Endocrinol 2011;7(12):738-48 «PMID: 21709707»PubMed
- Preshaw PM, Alba AL, Herrera D, ym. Periodontitis and diabetes: a two-way relationship. Diabetologia 2012;55(1):21-31 «PMID: 22057194»PubMed
- Sanz M, Ceriello A, Buysschaert M, ym. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J Clin Periodontol 2018;45(2):138-149 «PMID: 29280174»PubMed
- Pre-eklampsia - tutkimustiedosta kotimaiseen hoitosuositukseen. Lääketieteellinen Aikakauskirja Duodecim 2023;139(7):563-70
- Qiao Y, Wang Z, Li Y, ym. Rheumatoid arthritis risk in periodontitis patients: A systematic review and meta-analysis. Joint Bone Spine 2020;87(6):556-564 «PMID: 32593704»PubMed
- D'Aiuto F, Orlandi M, Gunsolley JC. Evidence that periodontal treatment improves biomarkers and CVD outcomes. J Periodontol 2013;84(4 Suppl):S85-S105 «PMID: 23631587»PubMed
- Teeuw WJ, Slot DE, Susanto H, ym. Treatment of periodontitis improves the atherosclerotic profile: a systematic review and meta-analysis. J Clin Periodontol 2014;41(1):70-9 «PMID: 24111886»PubMed
- Artese HP, Foz AM, Rabelo Mde S, ym. Periodontal therapy and systemic inflammation in type 2 diabetes mellitus: a meta-analysis. PLoS One 2015;10(5):e0128344 «PMID: 26010492»PubMed
- Luthra S, Orlandi M, Hussain SB, ym. Treatment of periodontitis and C-reactive protein: A systematic review and meta-analysis of randomized clinical trials. J Clin Periodontol 2023;50(1):45-60 «PMID: 35946825»PubMed
- Esteves Lima RP, Atanazio ARS, Costa FO, ym. Impact of non-surgical periodontal treatment on serum TNF-α levels in individuals with type 2 diabetes: a systematic review and meta-analysis. J Evid Based Dent Pract 2021;21(2):101546 «PMID: 34391555»PubMed
- Shah B, Shah M, Geisinger M, ym. Effect of non-surgical therapy on plasma C-reactive protein levels in patients with periodontitis: A single arm prospective clinical trial. J Periodontol 2023;94(3):336-343 «PMID: 36069212»PubMed
- Sun J, Zheng Y, Bian X, ym. Non-surgical periodontal treatment improves rheumatoid arthritis disease activity: a meta-analysis. Clin Oral Investig 2021;25(8):4975-4985 «PMID: 33515120»PubMed
- Molina A, Huck O, Herrera D, ym. The association between respiratory diseases and periodontitis: A systematic review and meta-analysis. J Clin Periodontol 2023;50(6):842-887 «PMID: 36606394»PubMed
- Fardal Ø, Grytten J. Applying quality assurance in real time to compliant long-term periodontal maintenance patients utilizing cost-effectiveness and cost utility. J Clin Periodontol 2014;41(6):604-11 «PMID: 24666095»PubMed
- Martin JA, Fardal Ø, Page RC, ym. Incorporating severity and risk as factors to the Fardal cost-effectiveness model to create a cost-benefit model for periodontal treatment. J Periodontol 2014;85(3):e31-9 «PMID: 24144268»PubMed
- Schwendicke F, Plaumann A, Stolpe M, ym. Retention costs of periodontally compromised molars in a German population. J Clin Periodontol 2016;43(3):261-70 «PMID: 27001032»PubMed
- Schwendicke F, Graetz C, Stolpe M, ym. Retaining or replacing molars with furcation involvement: a cost-effectiveness comparison of different strategies. J Clin Periodontol 2014;41(11):1090-7 «PMID: 25255893»PubMed
- Nagpal D, Ibraimova L, Ohinmaa A, ym. The cost-effectiveness of tooth preservation vs implant placement in severe periodontal disease patients: a systematic review. Quintessence Int 2024;55(1):76-85 «PMID: 37823844»PubMed
- Schwendicke F, Stolpe M, Plaumann A, ym. Cost-effectiveness of regular versus irregular supportive periodontal therapy or tooth removal. J Clin Periodontol 2016;43(11):940-947 «PMID: 27397850»PubMed
- Pattamatta M, Chapple I, Listl S. The value-for money of preventing and managing periodontitis: Opportunities and challenges. Periodontol 2000 2024 May 14 «PMID: 38745388»PubMed
- Needleman I, McGrath C, Floyd P, ym. Impact of oral health on the life quality of periodontal patients. J Clin Periodontol 2004;31(6):454-7 «PMID: 15142215»PubMed
- O'Dowd LK, Durham J, McCracken GI, ym. Patients' experiences of the impact of periodontal disease. J Clin Periodontol 2010;37(4):334-9 «PMID: 20447256»PubMed
- Salvi GE, Mischler DC, Schmidlin K, ym. Risk factors associated with the longevity of multi-rooted teeth. Long-term outcomes after active and supportive periodontal therapy. J Clin Periodontol 2014;41(7):701-7 «PMID: 24766602»PubMed
- Braegger U. Cost-benefit, cost-effectiveness and cost-utility analyses of periodontitis prevention. J Clin Periodontol 2005;32 Suppl 6:301-13 «PMID: 16128845»PubMed
- Gjermo PE. Impact of periodontal preventive programmes on the data from epidemiologic studies. J Clin Periodontol 2005;32 Suppl 6:294-300 «PMID: 16128844»PubMed
- Gaunt F, Devine M, Pennington M, ym. The cost-effectiveness of supportive periodontal care for patients with chronic periodontitis. J Clin Periodontol 2008;35(8 Suppl):67-82 «PMID: 18724842»PubMed
- Tomasi C, Wennström JL, Berglundh T. Longevity of teeth and implants - a systematic review. J Oral Rehabil 2008;35 Suppl 1:23-32 «PMID: 18181931»PubMed
- Holm-Pedersen P, Lang NP, Müller F. What are the longevities of teeth and oral implants? Clin Oral Implants Res 2007;18 Suppl 3:15-9 «PMID: 17594366»PubMed
- Pjetursson BE, Heimisdottir K. Dental implants - are they better than natural teeth? Eur J Oral Sci 2018;126 Suppl 1:81-87 «PMID: 30178552»PubMed
- Kupka JR, König J, Al-Nawas B, ym. How far can we go? A 20-year meta-analysis of dental implant survival rates. Clin Oral Investig 2024;28(10):541 «PMID: 39305362»PubMed
